





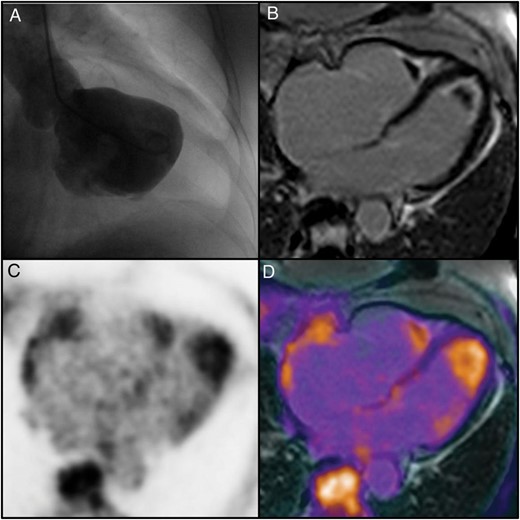
A 73-year-old woman presented with a 3-week history of progressive exertional dyspnoea and elevated cardiac enzymes. Cardiac catheterization revealed no coronary artery disease but thickening of the apical endocardium of the left ventricle despite nearly normal systolic function (Panel A). Differential blood count with marked peripheral blood eosinophilia (2 × 109/µL) led to the suspected diagnosis of Loeffler endocarditis. Owing to the potential risk of embolism, we refused to perform biopsy. Instead, the patient was scheduled for simultaneous positron emission tomography/magnetic resonance (PET/MR) imaging. To enhance inflammatory activity and suppress normal myocardial uptake of 18FDG, our patient received a high-fat, low-carbohydrate diet the day before and was fasted 12 h prior to imaging. Magnetic resonance depicted the typical pattern of late gadolinium enhancement (LGE) lesions restricted circumferentially to the endocardium within the apical region of both ventricles. Furthermore, it showed an apical mass in both ventricles without LGE, mostly complying with apical thrombi (Panel B). In contrast, simultaneous PET imaging yielded a strong 18FDG uptake not only in the LGE region, but particularly within the apical mass of both ventricles identifying the presence of active inflammatory tissue (Panels C and D). Loeffler endocarditis has been temporally divided into an early usually clinically silent acute necrotic, followed by a symptomatic thrombotic, and finally a late fibrotic stage. Hybrid PET/MR imaging of the heart is a promising non-invasive tool to provide the diagnosis and graduate the inflammatory activity of Loeffler endocarditis and may be valuable in monitoring the effect of anti-inflammatory therapy.
(Panel A) Left ventriculography showing thickening of the apical endocardium of the left ventricle. (Panel B) Magnetic resonance imaging in four-chamber orientation depicting late gadolinium contrast-enhanced (LGE) lesions restricted circumferentially to the endocardium within the apical region of both ventricles in contrast to an apical mass in the left and right ventricle without LGE. (Panel C) FDG-PET in four-chamber orientation demonstrating a strong 18FDG uptake within the whole-apical region of both ventricles. (Panel D) Fusion overlay of MRI and FDG-PET in four-chamber orientation, confirming 18FDG uptake not only in the LGE region but particularly within the apical mass of both ventricles identifying the presence of active inflammatory tissue.


{kind=link}