





Embolic brachial artery occlusion most often originates from the heart, the aortic arch, or from subclavian artery aneurysms.
A 64-year-old man presented with acute upper limb ischaemia of the left arm. Duplex sonography confirmed a brachial artery occlusion, but no compression of the left subclavian artery or a subclavian aneurysm as source for the emboli. There were no signs for cardiac arrhythmia in the ECG nor cardiac thrombus by echocardiography. Computed angiogram of the thoracic and upper extremity revealed an aneurysm of the left posterior circumflex humeral artery (Panels A and B). Treatment consists in surgical embolectomy at the brachial bifurcation and in ligation of the aneurysm.
Aneurysms of the posterior circumflex humeral artery have been reported for volleyball and baseball players and named as the ‘Pitcher Syndrome'. Repetitive traumas to the arterial wall during throwing motions of the shoulder affect the posterior circumflex humeral artery at the quadrangular space at the neck of the humerus. Embolic occlusion may result from dislocation of the squeezed thrombus from the aneurysmatic sack during shoulder movements. Since this patient did never practice any other sports than yoga, it might be assumed that certain specific yoga exercises with shoulder movements might have provoked the artery trauma.
The absence of cardiovascular source for thrombo-embolism by echocardiography, ECG, and vascular sonography demands additional vascular imaging that allows an entire vascular assessment to detect rare sources for embolism.
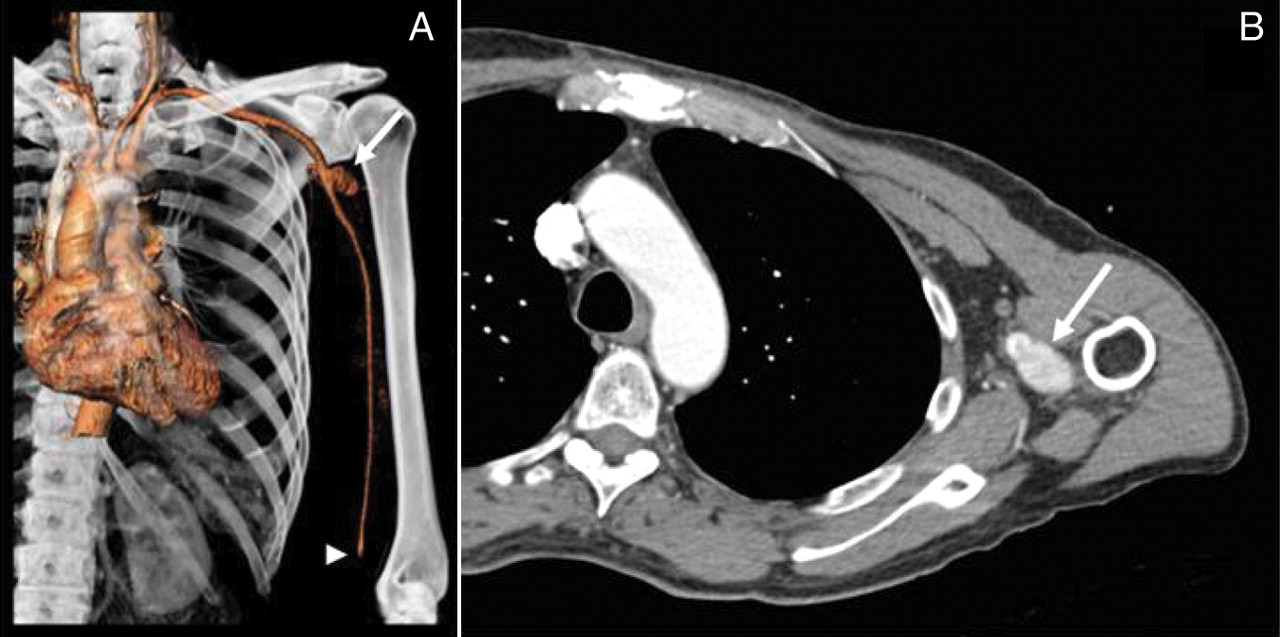
Panel A. Three-dimensional volume rendering computed tomography image. Aneurysm of the left posterior circumflex humeral artery (white arrow) and thromboembolic occlusion of the left brachial artery bifurcation (white arrowhead).
Panel B. Transverse computed tomography image. Aneurysm of the left posterior circumflex humeral artery (white arrow).


{kind=link}
{kind=link}