





In 1977 the term ‘cardiogenic dementia’ was coined, suggesting that this disorder might at least in some instances be secondary to cardiovascular disease (CVD).1 To date, various smaller studies have sought to clarify this issue, but results have not always been consistent. Since in the elderly, cognitive impairment (CI), CVD, and heart failure (HF) frequently co-occur, the precise mechanisms underlying CI have remained difficult to disentangle.
Neurobiology of important disorders such as depression and dementia has proposed exciting hypotheses,2 but has so far not thoroughly clarified the biological links with CVD. In experimental animals post-myocardial infarction, neurohumoral ‘remodelling’ was observed in multiple brain areas, and reduction of hypothalamic inflammation appeared to prevent heart failure.3,4 In humans, an association between the total burden of CVD and cognitive deterioration was reported.5,6 Further, the degree of CI correlated with the severity of left ventricular systolic dysfunction in HF patients.7 Reduced brain perfusion as a consequence of hypotension or low cardiac output was found to be implicated in cerebral dysfunction,8,9 and patients with impaired cerebrovascular reactivity due to old age, recent stroke, or carotid occlusive disease appeared at particular risk for brain ischaemia and atrophy due to hypoperfusion.10 Atrial fibrillation as a frequent complication of CVD and HF was found associated with both Alzheimer's disease and vascular dementia.11 Vice versa, cortical and autonomic nerve dysfunction and the brainstem appear also to affect cardiac electrophysiology and arrhythmias.12 Close associations between CI and other neuropsychological or functional perturbations, such as, for example, depression or sleep-disordered breathing, have been shown.13,14 On the other hand, variants of gene expression or activation of vasopressin, crucial for blood pressure regulation, and sodium and water regulation, were shown also to influence human social communication.15,16 Last, but not least, cardiovascular drugs may have central effects.17 Against this background, a multifactorial pathogenesis of CI seems likely, which might explain why the profiles of CI observed in different studies and patient populations have been heterogenous. Two recent clinical studies have now provided further evidence on the interrelationship of CVD and structural and functional brain disorders.
Standardized neuropsychological testing, echocardiography, and magnetic resonance brain imaging constitute appropriate and complementary methods to study CI pathophysiology. Building on their previous work,18 Almeida et al. report correlations of various domains of CI with quantitative measures of cerebral grey matter volume.19 Previous studies were of limited sample size and compared atrophy in selected target areas of the brain only in patients with overt systolic HF and healthy controls.20,21 The present study had a reasonable size, imaged the entire brain, and included patients with HF, healthy subjects, and an additional control group with ischaemic heart disease (IHD) only. Almeida et al. show that compared with healthy controls, HF patients had lower scores on several cognition variables such as immediate memory, long delay recall, and digit coding, and exhibited grey matter loss in various brain areas, indicating a significant loss of total cerebral grey matter volume. Notably, this loss was associated neither with physical capacity nor with left ventricular ejection fraction. Patients with IHD also had lower long delay scores compared with the healthy individuals and exhibited a relative loss of grey matter volume, but much less and much more circumscribed than the HF patients.
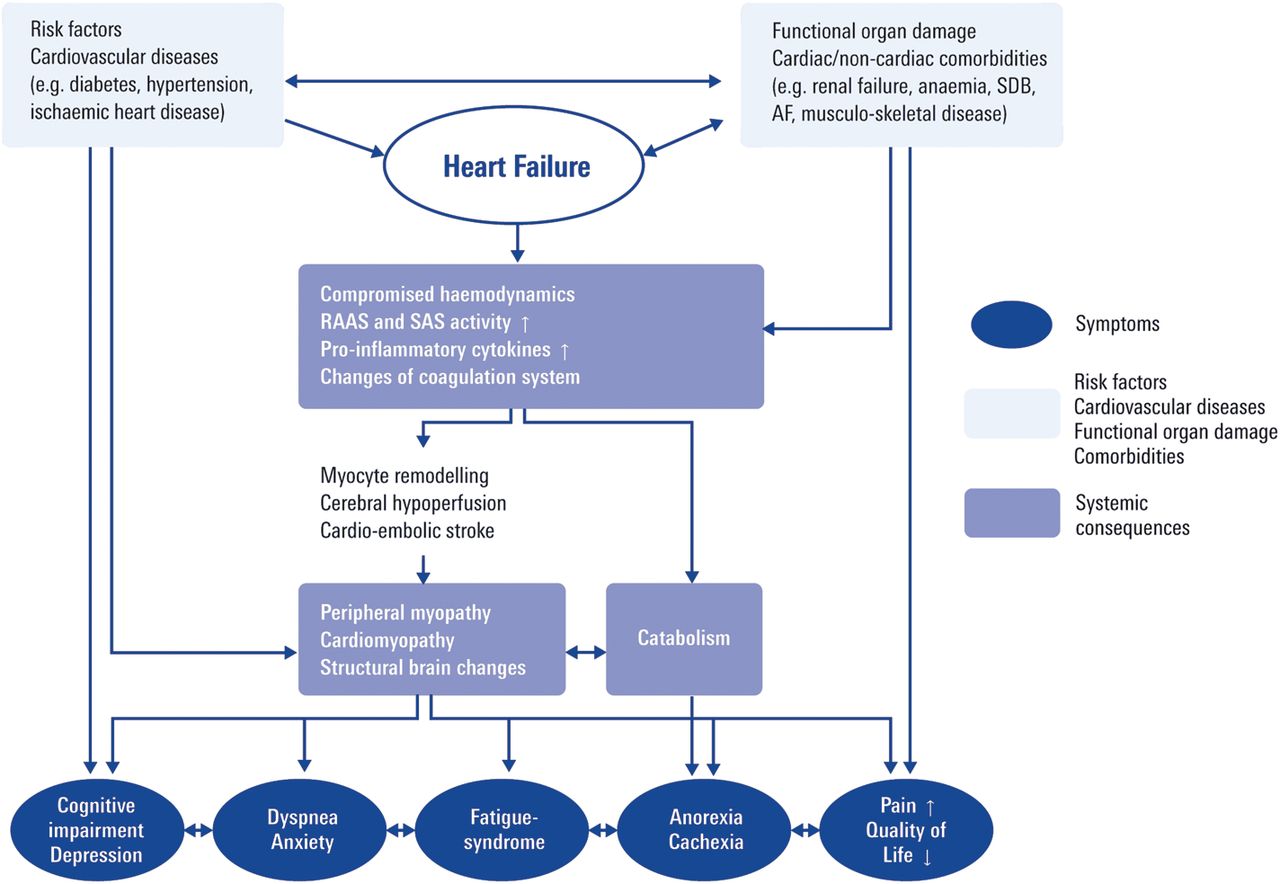
These data demonstrate that cognitive losses and morphological brain changes may occur solely as a sequel of risk factor and CVD burden in patients with normal pump function. It seems plausible that as CVD progresses to HF, additional pathogenetic mechanisms may become active (Figure 1) and lead to ischaemic damage and further brain matter losses in regions relevant to cognitive function. Although Almeida et al.19 do not provide data regarding disease duration, it may be hypothesized that the functional and morphological changes in HF patients vs. those in controls with only IHD reflect a disease continuum. With their work, the authors shed light on several important aspects of the complex CI pathophysiology. However, due to the relatively small number of subjects in the HF group, they could not attempt to study specific HF aetiologies, e.g. compare cardiomyopathies and IHD, in their potentially differential relationship to cerebral abnormalities. Further, they did not report how many patients had a previous clinical stroke, and did not assess cerebral blood flow or cardioembolic burden by imaging. Finally, the cross-sectional nature of the study precluded the determination of whether the observed cerebral and cognitive changes were progressive in nature, and in which way they impacted on outcome.
Possible interrelations among risk factors, cardiovascular diseases, co-morbidities, systemic consequences, and symptoms in the cardiovascular disease continuum. RAAS, renin–angiotensin–aldosterone system; SAS, sympathoadrenergic system; SDB, sleep-disordered breathing; AF, atrial fibrillation.
O'Donnell et al. provide complementary information, and answer some of the open questions.22 Based on scores derived from the Mini-Mental State Examination (MMSE), they determined in 30 959 patients (98.2% of the pooled samples of the ONTARGET and TRANSCEND populations) with a prior cardiovascular event or diabetes mellitus the association between CI and subsequent risk of cardiovascular events (composite endpoint: cardiovascular death, stroke, myocardial infarction, or hospitalization for HF). Patients were categorized into four groups according to baseline MMSE: 30, 29–27, 26–24, and <24. The main finding was a graded inverse association of the MMSE score with all components of the composite endpoint except myocardial infarction, and that this relationship was independent of all other prognostic factors investigated in this study. A score <24 was associated with a 35% relative increase in the risk of cardiovascular events, comparable with the risk conferred by a prior stroke or myocardial infarction. Importantly, participants exhibiting an MMSE decline by two or more points at follow-up after 2 years subsequently experienced more cardiovascular events than those without decline (12.1% vs. 8.8% after 2 years).
Although objective evidence of cerebral abnormalities by neuroimaging was not available, this study22 provides strong arguments that CI as indicated by a reduced MMSE score represents a marker of cerebrovascular damage in such high risk cardiovascular patients, since a prior history of clinical stroke or a stroke at follow-up was increasingly more common in these subjects. O'Donnell et al. were thus able to show that progression of CI may indeed occur over time, and that this most probably corresponds to a progression of structural cerebral abnormalities. Considering the very large sample size facilitating adjustment for a broad range of potentially confounding lifestyle risk factors, these data strongly suggest the adverse prognostic implications of CI in a broad spectrum of cardiovascular outcomes.
What are the practical implications of these reports? Almeida et al.19 propose that CI may be responsible for the low adherence of many HF patients to complex self-care regimens. Accordingly, screening for CI would seem desirable, and might perhaps enhance implementation of individualized care models, in which monitoring, education, and self-empowerment are tailored to patients' physical needs and mental capabilities. If patients were enabled to engage in consistent self-care, outcomes might be improved and healthcare utilization and costs reduced. O'Donnell et al.22 advocate that patients with CI require aggressive vascular risk factor modification, comparable with other secondary prevention populations. Positive effects of physical training on cognitive performance have recently been reported from the HF-action trial,23 and strengthen this concept.
Functional impairment of other organs, such as the kidney, the lungs, or the bone marrow, and cardiac and non-cardiac co-morbidities are frequent in CVD and HF, and modulate the patients' individual symptom profiles. Evidence is growing that both the number of co-morbid conditions and the severity of symptoms impact on disease progression and prognosis. Whether specific therapies targeting the improvement of individual facets of the complex derangement implicated in the cardiovascular continuum (Figure 1) may reverse CI or at least prevent progression requires further research. Cardiac transplantation and ventricular resynchronization therapy have been shown to improve psychological distress and several domains of cognitive functioning significantly,24,25 but patient numbers were small, and not all publications confirm these positive results.26,27 Experimental studies and data obtained in hypertensive patients support the concept that brain-penetrating inhibitors of the renin–angiotensin–aldosterone system may, by inhibiting degradation of certain neurotransmitters, exert positive effects on cognitive function.17 Kindermann et al. report in a recent publication that in patients with decompensated HF several indices of cognition, but also depression, improved significantly after appropriate HF pharmacotherapy and stabilization of functional status.28 This would indicate that at least in the acute state, partial remission of CI might be attained. Moreover, a close association between depression and CI13 and favourable effects of improvement of these neuropsychological perturbances on self-reported adherence to medication and health behaviours29 were recently demonstrated.
Thus, there is unequivocal evidence that cognition matters in CVD and HF. The MMSE is a well established and simple cognitive screening test, which cardiologists should consider including in their diagnostic tool box in order to better identify subjects at increased risk and be able to adjust therapeutic strategies to their patients' cognitive abilities.
Conflict of interest: none declared.
References
Author notes
The opinions expressed in this article are not necessarily those of the Editors of the European Heart Journal or of the European Society of Cardiology.
†doi:10.1093/eurheartj/ehr467
‡doi:10.1093/eurheartj/ehs053.


{kind=link}
{kind=link}