





Abstract
Invasive cardiologists are the most exposed to ionizing radiation among health professionals and show an increased rate of somatic DNA damage. To evaluate the effects of chronic low-dose exposure to ionizing radiation on redox state and apoptotic activation.
We enrolled 10 healthy exposed professionals (all interventional cardiologists, Group II, exposed: age = 38 ± 5 years) and 10 age- and gender-matched unexposed controls (Group I, non-exposed). Exposed subjects had a median exposure of 4 mSv/year (range 1–8) by film badge dosimetry (below lead apron). We measured reduced glutathione (GSH, a marker of antioxidant response) in erythrocytes and plasma generation of hydrogen peroxide (a marker of oxyradical stress) by ferrous oxidation-xylenol orange assay in plasma. In both groups, lymphocytes were isolated and caspase-3 activity (a marker of apoptotic response) measured at baseline and following 2 Gy in vitro irradiation. Exposed subjects showed a three-fold increase in hydrogen peroxide (Group I = 2.21 ± 1.03 vs. II = 6.51 ± 1.55 μM H2O2 equivalents) and a 1.7-fold increase in GSH (I = 12.37 ± 1.22 vs. II = 20.61 ± 2.16 mM). Exposed subjects also showed higher values of caspase-3 activity, both at baseline and—more strikingly—following high-dose radiation challenge.
In interventional cardiologists, chronic exposure to low-dose radiation is associated with an altered redox balance mirrored by an increase in hydrogen peroxide and with two possibly adaptive cellular responses: (i) an enhanced antioxidant defence (increase in GSH, counteracting increased oxyradical stress) and (ii) an increased susceptibility to apoptotic induction which might efficiently remove genetically damaged cells.
Introduction
Recently, there has been a growing concern from advisory bodies on the unprecedented level of professional exposure in interventional cardiologists.1,2 Invasive cardiology procedures increased 10-fold in the last 10 years in both Europe and the USA, with concomitant concerns for the safety of the staff directly involved in such relatively strong radiation procedures. Interventional cardiologists have an exposure per head per year 2–3 times higher than that of radiologists, and this exposure has increased steadily in the past 20 years.3,4 They represent today perhaps one of the best possible human model to assess the biological effects of chronic exposure to low-dose radiation (LDR).5
Recent studies suggest that cumulative professional radiological exposure is associated with a non-negligible lifetime attributable risk of cancer for the most exposed contemporary cardiac catheterization laboratory staff.6 This risk might be associated with an increased micronuclei frequency for interventional cardiologists, but not for clinical cardiologists, which correlates with years of professional activity.7 On the other side, dated evidence suggest that LDR, induced by very low doses of X-rays, can make human lymphocytes less susceptible to the genetic damage manifested as chromatid breakage induced by a subsequent high dose of X-rays.8–10 This phenomenon is an example of ‘radiation adaptive response’ which have been often evoked as possible mechanisms to stimulate certain protective functions, including antioxidant capacity, DNA repair mechanisms, and apoptosis.11–15
Basic studies on the mechanisms of biological response to radiation at low doses are considered a research priority in order to better understand the occupational risks associated with working in a catheterization laboratory with the possible development of long-term health effects. Here, we analysed the response to chronic LDR exposure of a group of interventional cardiologists measuring haematological changes of redox state [reduced glutathione (GSH) in erythrocytes as a marker of antioxidant response and plasma generation of hydrogen peroxide as a marker of oxyradical stress] and increased sensitivity to apoptosis (caspase-3 activity) in lymphocytes, at baseline and following 2 Gy in vitro irradiation.
Methods
Subjects
We enrolled 10 healthy exposed professionals (all interventional cardiologists, Group II, exposed: age = 38 ± 5 years) and 10 age- and gender-matched unexposed controls (Group I, unexposed) (Table 1). The exposed group included all physicians working in the catheterization unit, while unexposed subjects were recruited among laboratory and hospital workers who did not have radiation exposure. Cholesterol, HDL cholesterol, triglycerides, and blood pressure values in the two groups were in the normal range (data not shown). By film badge dosimetry, exposed subjects had a median exposure of 4 mSv for the last year (range 1–8) (Table 1). In all exposed subjects, a lifetime dosimetric reconstruction was obtained from the local Health Physics data bank.6 According to ICRP 6016 and European Commission Directive,17 radiation dose to workers was expressed as an effective dose in milliSievert (mSv) calculated from personal equivalent thermoluminescent dosimetry, at the waist or chest, under apron, following recommendations of the National Council of Radiation Protection.18
Characteristics of the examinees
| Unexposed (Group I) | Exposed (Group II) | P-value | |
|---|---|---|---|
| Mean age (years) | 35 ± 3 | 38 ± 5 | 0.530 |
| Gender [n (%)] | |||
| Male | 8 (80) | 10 (100) | 1.00 |
| Female | 2 (20) | 0 (0) | |
| Body mass index | 22 ± 2 | 26 ± 2 | 0.010 |
| Alcohol consumption | 0/10 | 1/10 | 1.00 |
| Smoking habit | 1/10 | 2/10 | 1.00 |
| Dietary style | National cuisine | National cuisine | |
| Supplements | No | No | |
| Dose (mSv/year) | 0 | 4.7 ± 3.2 | |
| Range | 0 | 1.2–8.3 | |
| Years of exposure | 0 | 10 ± 6 | |
| Range | 0 | 3–19 | |
| Number of procedures | 0 | 525 ± 100 | |
| Range | 0 | 250–750 | |
| Unexposed (Group I) | Exposed (Group II) | P-value | |
|---|---|---|---|
| Mean age (years) | 35 ± 3 | 38 ± 5 | 0.530 |
| Gender [n (%)] | |||
| Male | 8 (80) | 10 (100) | 1.00 |
| Female | 2 (20) | 0 (0) | |
| Body mass index | 22 ± 2 | 26 ± 2 | 0.010 |
| Alcohol consumption | 0/10 | 1/10 | 1.00 |
| Smoking habit | 1/10 | 2/10 | 1.00 |
| Dietary style | National cuisine | National cuisine | |
| Supplements | No | No | |
| Dose (mSv/year) | 0 | 4.7 ± 3.2 | |
| Range | 0 | 1.2–8.3 | |
| Years of exposure | 0 | 10 ± 6 | |
| Range | 0 | 3–19 | |
| Number of procedures | 0 | 525 ± 100 | |
| Range | 0 | 250–750 | |
Characteristics of the examinees
| Unexposed (Group I) | Exposed (Group II) | P-value | |
|---|---|---|---|
| Mean age (years) | 35 ± 3 | 38 ± 5 | 0.530 |
| Gender [n (%)] | |||
| Male | 8 (80) | 10 (100) | 1.00 |
| Female | 2 (20) | 0 (0) | |
| Body mass index | 22 ± 2 | 26 ± 2 | 0.010 |
| Alcohol consumption | 0/10 | 1/10 | 1.00 |
| Smoking habit | 1/10 | 2/10 | 1.00 |
| Dietary style | National cuisine | National cuisine | |
| Supplements | No | No | |
| Dose (mSv/year) | 0 | 4.7 ± 3.2 | |
| Range | 0 | 1.2–8.3 | |
| Years of exposure | 0 | 10 ± 6 | |
| Range | 0 | 3–19 | |
| Number of procedures | 0 | 525 ± 100 | |
| Range | 0 | 250–750 | |
| Unexposed (Group I) | Exposed (Group II) | P-value | |
|---|---|---|---|
| Mean age (years) | 35 ± 3 | 38 ± 5 | 0.530 |
| Gender [n (%)] | |||
| Male | 8 (80) | 10 (100) | 1.00 |
| Female | 2 (20) | 0 (0) | |
| Body mass index | 22 ± 2 | 26 ± 2 | 0.010 |
| Alcohol consumption | 0/10 | 1/10 | 1.00 |
| Smoking habit | 1/10 | 2/10 | 1.00 |
| Dietary style | National cuisine | National cuisine | |
| Supplements | No | No | |
| Dose (mSv/year) | 0 | 4.7 ± 3.2 | |
| Range | 0 | 1.2–8.3 | |
| Years of exposure | 0 | 10 ± 6 | |
| Range | 0 | 3–19 | |
| Number of procedures | 0 | 525 ± 100 | |
| Range | 0 | 250–750 | |
Reagents
Glutathione; phthaldialdehyde, trichloroacetic acid; hydrogen peroxide; tert-butyl hydroperoxide; 2,2′-azino-bis(3-ethylbenz-thiazoline-6-sulfonic acid) (ABTS); butylated hydroxytoluene; 3,3′-bis[N,N-bis(carboxymethyl)aminomethyl]-o-cresolsulfonephthalein tetrasodium salt (Xylenol Orange); ammonium ferrous sulfate were from Sigma-Aldrich Chemical Co. (Milan, Italy); sodium azide from AppliChem GmbH (Darmstadt, Germany); and dichlorofluorescein-diacetate (DCFA) and phosphate-buffered saline (PBS) tablets were purchased from Invitrogen (S. Giuliano Milanese, Milan, Italy). All other chemicals used were of research highest purity grade.
Sample preparation
Blood samples were drawn into glass tubes containing EDTA from the femoral arterial sheaths. Red blood cells were separated from plasma by centrifugation at 3000 g at 4°C for 30 min, washed three times with PBS to remove the buffy coat. Alternatively, 6 mL of venous blood was drawn into a glass tube without any anticoagulant to obtain serum samples after centrifugation. Haemolysates were prepared by incubating freshly erythrocytes with cold distilled water followed by microcentrifugation at 1300 g for 10 min. Haemolysis was determinate by spectrophotometric measurement at 540 nm. Mononuclear cells were isolated from peripheral blood. Following density-gradient centrifugation (Ficoll-Paque Plus; GE Healthcare, Milan, Italy), cells were washed three times in PBS, counted with Trypan Blue dye to assess their viability (cell viability >95%) and were immediately cultured as reported.19
Enzymatic and non-enzymatic glutathione, reactive oxygen species, superoxide dismutase, and catalase assays
The serum total antioxidant capacity was determined by colorimetric measurement using ABTS radical cation as a substrate.20 Hydrogen peroxide levels on plasma were measured in all subjects by the ferrous oxidation-xylenol orange assay as described previously.21 Fluorescent measurement of intracellular reactive oxygen species (ROS) was conducted by using permeant and non-fluorescent DCFA.22
Glutathione content in erythrocytes was determined on haemolysates using phthaldialdehyde as a substrate.23 Catalase (CAT) and superoxide dismutase (SOD) enzymatic activities were measured on haemolysates by a spectrophotometric method24 and a commercially available kit (Cayman Chemical Co., Ann Arbor, MI, USA), respectively.
Caspase-3 activity
For caspase-3 enzymatic activity, isolated lymphocytes (1 × 106/mL) were incubated for 3 h in RPMI, 10% FBS. At the end of incubation, we measured caspase-3 activity at baseline and following 2 Gy (200 rad) in vitro irradiation (GAMMACELL 1000 Elite; MDS Nordion, Ottawa, Canada). Cells were washed twice in PBS and suspended in lysis buffer (10 mM Hepes, pH 7.4; 2 mM ethylenediaminetetraacetic acid; 0.1% 3-[(3-cholamidopropyl)dimethylammonio]-1-propanesulfonate (CHAPS); 5 mM dithiothreitol; 1 mM phenylmethylsulfonylfluoride; 10 µg/mL pepstatina-A; 10 µg/mL apronitin; 20 µg/mL leupeptin). Following measurement of protein concentration, cell extracts were added with reaction buffer and the respective conjugated AFC (amino-4-trifluorometyl coumarin) substrate, Z-DEVD-AFC (carbobenzoxy-Asp-Glu-Val-Asp and Leu-Glu-Hys-Asp) before incubation at 37°C for 30 min. Upon proteolytic cleavage of the substrates by caspase-3, the free fluorochrome AFC was detected by a spectrofluorimeter multiplate reader (FL-500 Bio-Tek Instruments, AHSI, Milan, Italy) with an excitation and emission setting of 395 ± 20 and 530 ± 20 nm respectively. To quantify enzymatic activities, an AFC standard curve was determined. Caspase-3 specific activity was measured as nmoles of AFC produced/min/mg proteins at 37°C at saturating substrate concentrations (50 μM).25
Statistical analysis
As variables of interest were normally distributed, data were expressed as mean ± SD and comparison between groups was carried out by two-sided Student's t-test. P-values <0.05 were considered significant. Statistical analyses were performed using Systat Software 7.01. The sample was large enough to provide at least 80% power to detect at P < 0.05 a 50% difference between cases and controls with regard to the three main outcomes of interest, that is, the level of plasma hydrogen peroxide, the GSH concentration in erythrocytes, and the basal level of caspase-3 activity in lymphocytes.
Results
Demographic characteristics of the study subjects are shown in Table 1. Exposed and control groups had comparable baseline characteristics, including age, sex, and smoking status.
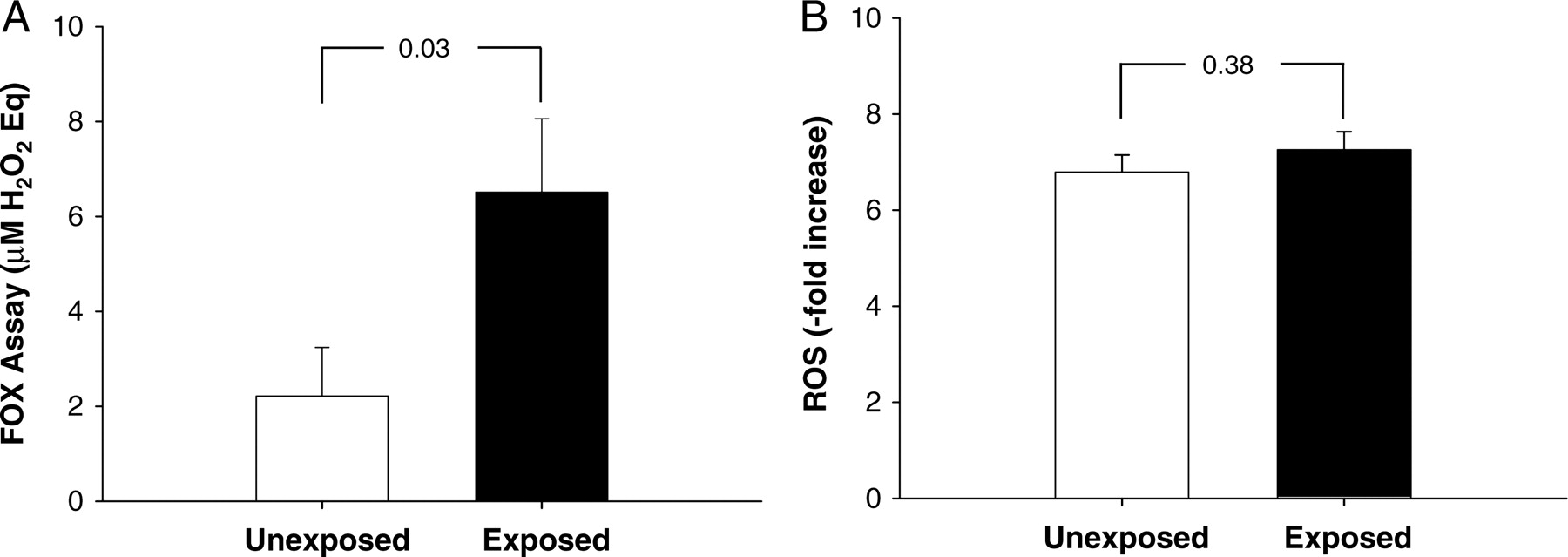
Exposed subjects showed a three-fold increase in hydrogen peroxide compared with the unexposed subjects (Group I = 2.21 ± 1.03 vs. II = 6.51 ± 1.55 μM H2O2 Eq) (Figure 1A). As a result of high increase in hydroxyl radical species, it would be expected to observe a different antioxidant level in the sera of the exposed subjects vs. the controls. However, as reported in Figure 2A, the total serum antioxidant power in the two groups did not show any significant change, suggesting a possible generation of adaptive response(s) in the exposed subjects able to counteract the ROS increase by activating antioxidant defence mechanisms.
Oxidative stress in non-exposed vs. exposed subjects. (A) Hydrogen peroxide concentration was measured by ferrous oxidation-xylenol orange assay and expressed as μM equivalent of H2O2 in plasma of cardiologists chronically exposed to low-dose radiation (black bar) in comparison to a control group of unexposed subjects (white bar). Data are expressed as mean ± SD (n = 10, P < 0.05). (B) Fluorescent measurement of intracellular reactive oxygen species was measured by using dichlorofluorescein-diacetate and expressed as a ratio between the fluorescent value after 10 min of 100 μM tert-butyl hydroperoxide exposure vs. basal in erythrocytes of cardiologists chronically exposed to low-dose radiation (black bar) in comparison to a control group of unexposed subjects (white bar). Data are expressed as mean ± SD (n = 10, P was not significant).
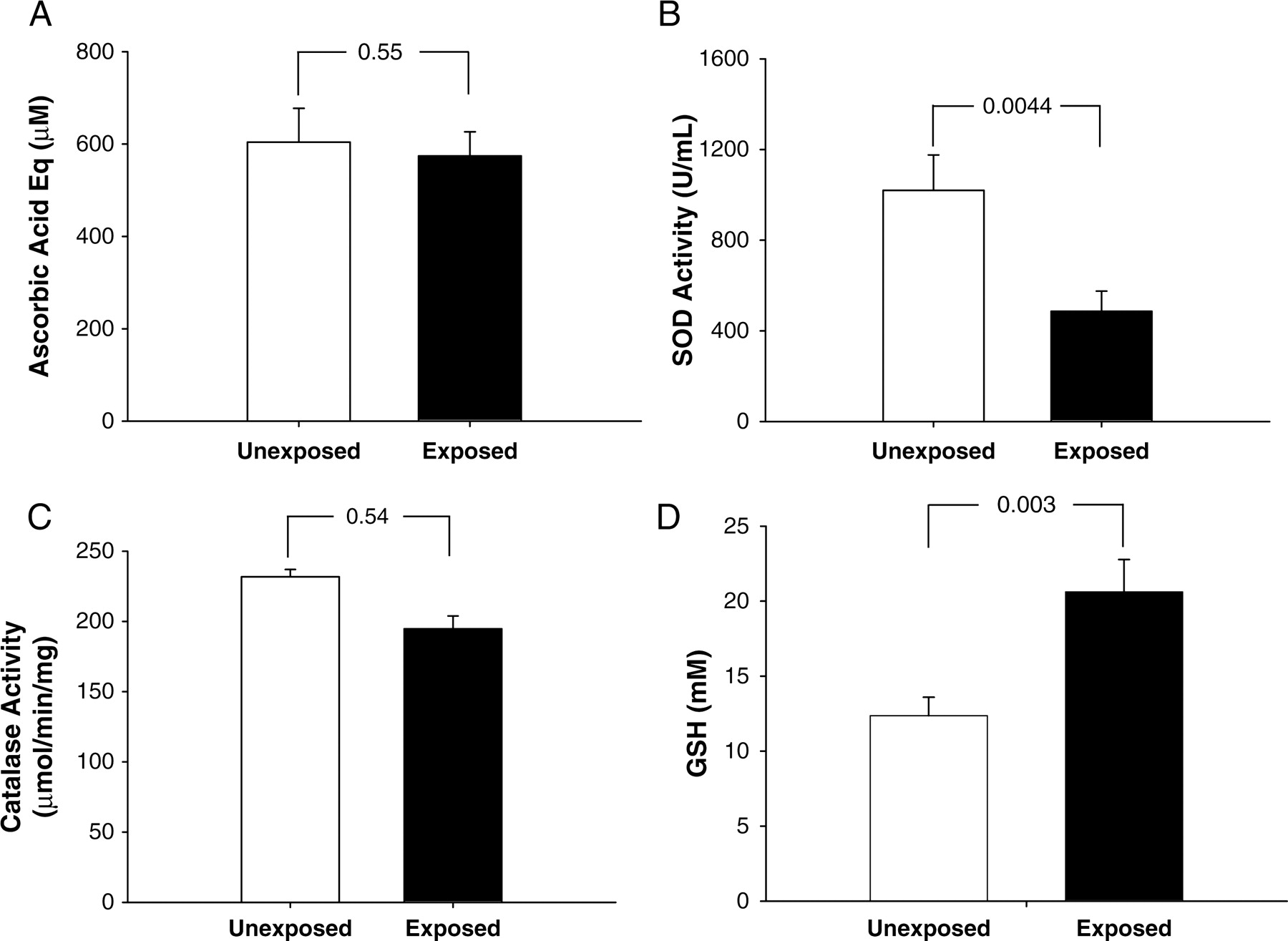
Antioxidant systems in non-exposed vs. exposed subjects. (A) Serum total antioxidant capacity was determined by colorimetric measurement using ABTS as a substrate and expressed as μM equivalent of ascorbic acid in cardiologists chronically exposed to low-dose radiation (black bar) in comparison to a control group of unexposed subjects (white bar). Data are expressed as mean ± SD (n = 10, P was not significant). Superoxide dismutase (SOD; B) and catalase (CAT; C) enzymatic activities were measured as reported in the Methods section in haemolysates prepared from cardiologists chronically exposed to low-dose radiation (black bars) in comparison to a control group of unexposed subjects (white bars). Data are expressed as mean ± SD (n = 10, P < 0.05 for SOD activity and not significant for CAT activity). (D) Glutathione content was determined on haemolysates of cardiologists chronically exposed to low-dose radiation (black bar) in comparison to a control group of unexposed subjects (white bar) using phthaldialdehyde as a substrate. Data are expressed as mean ± SD (n = 10, P < 0.05).
According to the literature, enzymatic and non-enzymatic pathways exist in human red cells to scavenge and detoxify ROS. The two main systems are represented by the SOD/CAT and GSH/GSH peroxidase (reviewed in Cimen26). The activity of Cu,Zn-SOD in erythrocytes of exposed subjects was significantly lower compared with unexposed (Figure 2B). The difference in enzymatic activity was not due to changes in the level of expression since immunoblotting showed comparable amount of SOD in the two groups (data not shown). The limited contribution of SOD in getting rid of ROS in exposed subjects was confirmed by the absence of significant differences in the activity of CAT in the two study groups (Figure 2C). On the opposite, differences between exposed and unexposed subjects were observed when measuring the level of GSH. In erythrocytes, GSH is the major antioxidant which protects important proteins such as spectrin;26,27 in addition, GSH is also part of the adaptive response induced by LDR.28,29 Glutathione was chosen as an antioxidant marker since it has direct radical-scavenging ability and its levels of erythrocyte GSH may reflect the GSH activity in other tissues.30 As shown in Figure 2D, GSH concentration increased of 1.7-fold in the exposed group and this change was significant (Group I = 20.61 ± 2.16 vs. II = 12.37 ± 1.22 μM). There was no correlation between GSH levels in erythrocytes and either last year radiation exposure or years of cath lab activity (data not shown). We finally measured the level of total ROS in erythrocytes of both groups. As a result of a balance between the oxidative stress produced by LDR (Figure 1A) and antioxidant defences activated by erythrocytes (Figure 2D), we did not detect any significant differences in ROS levels (Figure 1B).
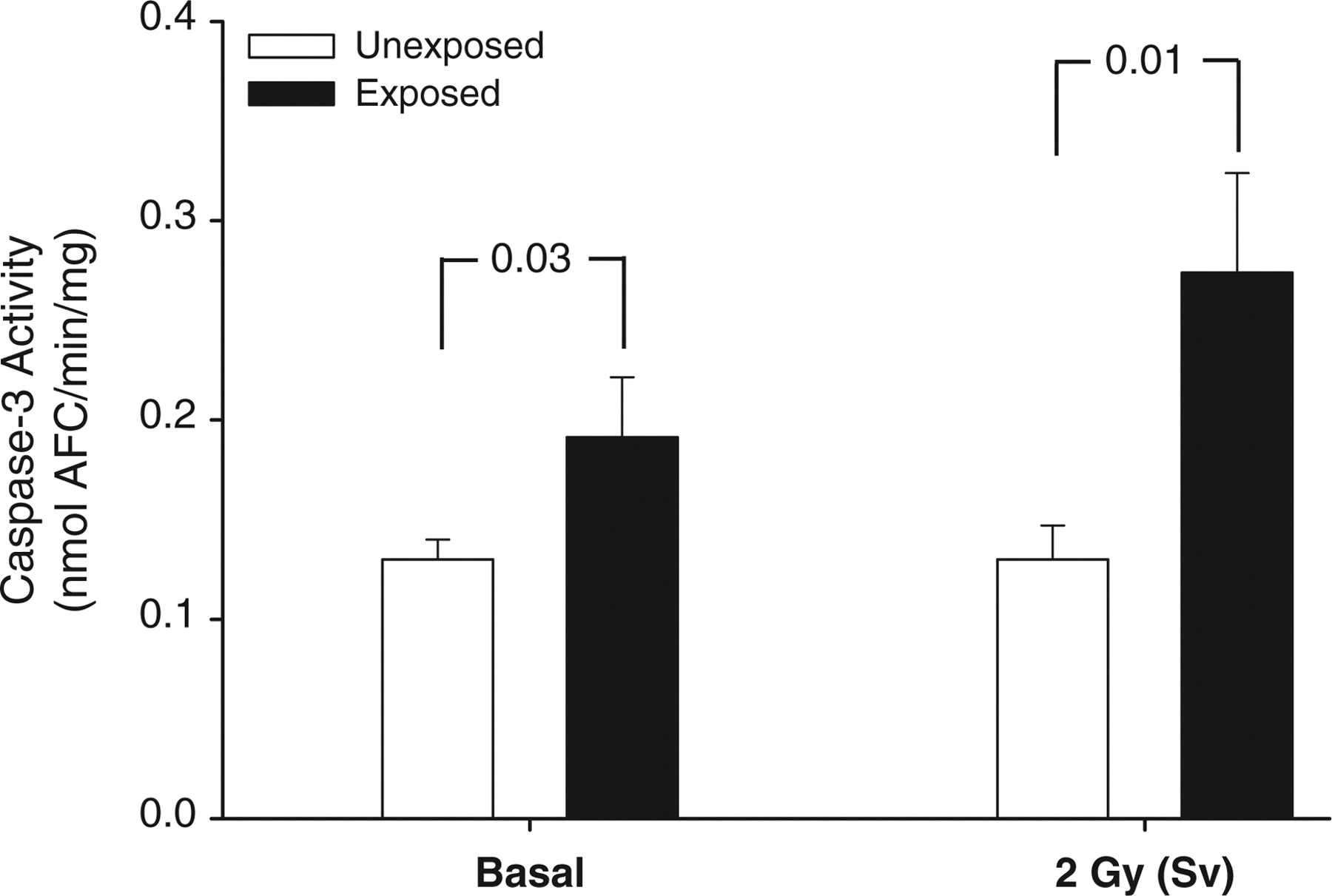
Circumstantial evidence suggest that the induction and magnitude of the adaptive response in human lymphocytes varies among people and depends on several factors including occupational exposure and genetic variability.18 Apoptosis may represent an important mechanism by which LDR induces an adaptive response in both normal31 and malignant cells.32 Since apoptosis is also strongly induced by redox imbalance, we measured, in the exposed cardiologists, the activity of caspase-3, a downstream effector of apoptotic processes. As reported in Figure 3, the basal level of caspase-3 was significantly increased in Group II (exposed); this effect was even more evident when lymphocytes were in vitro irradiated with an acute dose of γ-ray (2 Gy). It is worthwhile to note that cells isolated from both exposed and not-exposed groups did not show any morphological sign of apoptosis (data not shown). There was no correlation between caspase-3 activity in lymphocytes and either last year radiation exposure or years of cath lab activity (data not shown).
Caspase-3 activity was measured on isolated lymphocytes of cardiologists chronically exposed to low-dose radiation (black bars) in comparison to a control group of unexposed subjects (white bars) at baseline and following 2 Gy in vitro irradiation as described in the Methods section. Data are expressed as mean ± SD (n = 10, P is indicated in the graph).
Discussion
The effective annual dose ranged from 1.5 to 8.4 mSv, corresponding to the average dose equivalent of 200 (range 75–440) chest X-rays per head per year. The lifetime exposure ranged between 20 and 100 mSv (from 1000 to 5000 chest X-rays). These doses, although below the maximal allowable limits set by the International Commission of Radiation Protection, can have clear biological and biochemical effects, as suggested here by the increased level of circulating ROS. A limitation of the study is that the wearing of radiation badges is subject to the user's capacity of remembering to put the badge on, and we did not have an estimation of the compliance for wearing of radiation badges. It is known that one-third of catheterization laboratory staff is negligent in wearing the dosimeters, which may represent a source of significant underestimation of calculated risk.33 In addition, reliable data on dosimetric exposure were only available for the last year, and the lifetime exposure could only be estimated very indirectly from years of cath lab work and the average number of procedures per year performed by each cardiologist.
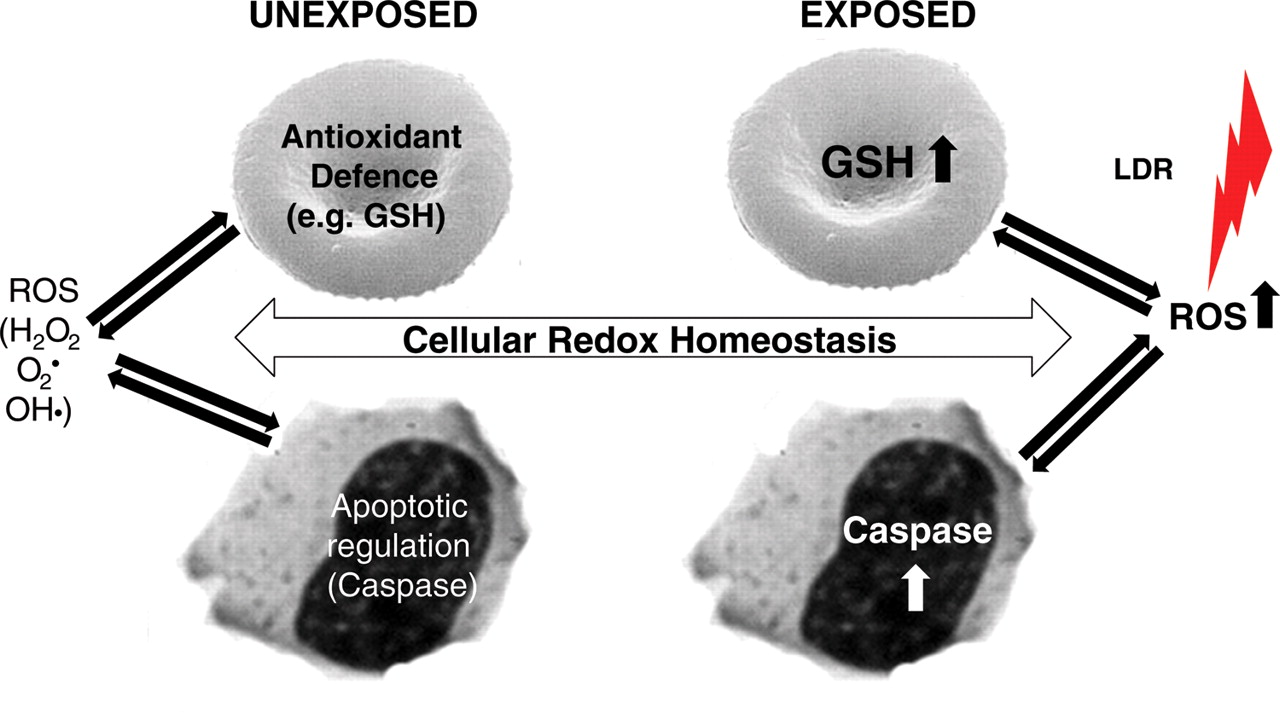
Our study demonstrated for the first time in interventional cardiologists that chronic exposure to LDR induces at least two physiological adaptive responses: an enhanced antioxidant defence (increased GSH levels in red cells), and an increased baseline level of caspase-3 activity (lymphocytes). Both mechanisms, in different ways, may compensate for the unbalanced ROS and contribute to maintain cellular homeostasis (summarized in the scheme reported in Figure 4). We hypothesized that in lymphocytes of the exposed group, LDR does not increase caspase-3 activity over the threshold necessary to induce apoptosis (Figure 4).
Schematic representation of the effect of low-dose radiation in interventional cardiologists accordingly to date reported in the text. In normal subjects (unexposed), the cellular redox homeostasis is maintained by a delicate equilibrium between reactive oxygen species production (endogenous and exogenous) and counteracting activity of antioxidant systems (enzymatic and non-enzymatic). Apoptosis may play a key role in this process since increased reactive oxygen species may lead to cell death. Prolonged exposure to low-dose radiation (interventional cardiologists) generates an increase in reactive oxygen species production which, in erythrocytes, is balanced by over-production of glutathione, while, in lymphocytes, this event increases the baseline level of caspase-3 without reaching the threshold necessary to induce apoptosis. Both defence mechanisms ensure redox balance in exposed subjects.
As a consequence of their physiological role, erythrocytes are exposed to continuous oxidative stress deriving from endogenous26 or exogenous sources, as in the case of professional exposure to radiation. For these reasons, red cells have developed efficient enzymatic and not-enzymatic antioxidant defences not only to preserve themselves from oxidative damage, but, due to their mobility, erythrocytes can be considered an ideal antioxidant acting as an oxidant scavenger throughout the circulation and reducing the damaging mass effect of large quantities of ROS on different tissues.34 These considerations represent the rationale for the investigation of antioxidant defences in erythrocytes of interventional cardiologists presented in this study. Our data suggest an efficient antioxidant response associated with increased production of GSH, the major antioxidant in red cells, in the exposed population which is probably sufficient to balance the increased ROS production due to LDR and maintaining their intracellular concentration constant (Figure 2). On the opposite, the SOD/CAT system seems to be involved in this defence mechanism. From a molecular point of view, the significant decrease in Cu,Zn-SOD enzymatic activity without changes in its expression in the group of interventional cardiologist represents an interesting observation which deserves further investigation actually in progress. It is worthwhile to note that other authors reported decreased activity of SOD in worker occupationally exposed to LDR.35 In a study examining a group of medical workers exposed to ionizing radiation, no significant differences were detected in the content of GSH vs. controls. In this case, the explanation compared with our data may reside in the observation that GSH was not measured in erythrocytes, but in the plasma of the examinees.29
Several mechanisms have been enacted by cells and organism to counteract the effects of ionizing radiations. Apoptosis, including programmed cell death, is a process in which a cell terminates itself by the destruction of vital cellular components or DNA via various molecular signalling pathways. In apoptosis, cells condense and fragment into membrane-bound apoptotic bodies, which are then ingested by phagocytes of the immune system for clearance.36,37 Medium- and high-dose radiations have been described to induce substantial levels of unrepairable, cellular damage leading to apoptosis.38 Adaptive responses induced by LDR have been observed in haematopoietic and immune systems, as shown by stimulatory effects on cell growth and resistance to subsequent radiation-induced cytogenetic damage.31 However, in terms of cell death by apoptosis, the effects of LDR are controversial. Some studies showed decreased apoptosis in response to LDR while others showed increased apoptosis. This controversy may be related to the radiation doses or dose rates, to the cell types, or to the species under investigation.32,39,40 Modifications of the complex intercellular ROS-based signalling system may also lead to configurations in which LDR attenuates ROS-mediated apoptosis induction.32 A key issue in the present study is that the population of exposed subjects is healthy, despite the level of exposure. The higher apoptotic threshold of their lymphocytes, at baseline and following high-dose radiation, can act as a double-edged sword: it is deleterious if it accelerates apoptosis in healthy cells. However, this does not seem to be the case in the present study, since the lymphocytes we analysed did not present any sign of apoptosis, nor the exposed cardiologists actually manifested any apoptosis-related disorders. Alternatively, an increased basal level of caspase-3 may predispose cells to genetic damage thus avoiding oncogenic effects, by removing potentially malignant somatic cells that contain a certain type and amount of DNA damage.7 In support of our data, it is worthwhile to mention that peripheral blood lymphocytes after a 5 Gy γ-irradiation showed a weak caspase-3 activation.41 On the opposite, cell lines with a functional p53 status showed high sensitivity to LDR resulting in increased apoptosis.42 However, others reported that low LET radiation induces a death response which has many characteristics of apoptosis but is p53-independent.43 Overall, these evidence suggest that the cellular proliferative status is an important determinant in response to LDR.
The unprecedented radiation exposure of the interventional cardiologists and staff in the cardiac catheterization laboratory represents a challenge and an opportunity for the cardiology community. Now, it is becoming increasingly clear that long-term radiation-induced cancer risk can be dramatically minimized by effective implementation of good practice of radiation protection in the catheterization laboratory,44 and ‘responsibility is on all physicians to minimize the radiation injury hazard to their patient, to their professional staff, and to themselves’.45
It is also an opportunity, since highly exposed interventional cardiologists are a suitable, perhaps unique model to understand the still elusive mechanisms of biological adaptation to chronic exposure to LDR. The finding of the present study clearly emphasize that a level of radiation exposure which is considered ‘safe’ by regulatory standards can induce a profound biochemical and cellular adaptation, of still uncertain clinical meaning, which must be understood to implement—if needed—appropriate countermeasures, from reduced exposure to chemoprophylaxis.
Funding
This work was supported by funding from Intercardioreprostudy grant of A.N.M.C.O. (Italian Association of Hospital Cardiologists) foundation to Institute of Clinical Physiology of National Research Council (Pisa, Italy).
Conflict of interest: none declared.
Acknowledgements
The exposed and unexposed subjects described in this article provided permission for their clinical information to be included. We thank the following colleagues for their contribution and advices toward the completion of this study: Drs Paolo Rubino and Valentina Picano from Clinica Cardiologica ‘Montevergine’, Mercogliano (Avellino, Italy); Dr Annunziata Nappo, Alfonso Siani, and Gianvincenzo Barba from Institute of Food Sciences, National Research Council (Avellino, Italy).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments
Editors, I cannot agree with the too generic statement of paper conclusion (1). As a matter of facts, not all "cardiologists", are created equal! I mean that the Authors ignore both Quantum Biophysical-Semeiotic Constituions, and their related Inherited Real Risks, I have discovered and described in larger Literature (2-17). For instance, regarding type 2 DM and Cancer, solid and liquid, a 55 year -long, well-established, clinical experience allows me to state that either ignoring or overlooking the real existence of Quantum Biophysical Semeiotic Constitutions, including diabetic Constitution and Oncological Terrain (http://www.semeioticabiofisica.it), as well as related Inherited Real Risks, bedside evaluated in a quantitative way, we cannot prevent and diagnose type 2 DM and cancer promptly, even in initial stage, bringing about an overlooked today's epidemics: Psychological Jatrogenetic Terrorism (2-5). In fact, authors around the world are thinking wrongly that ALL individuals are born equal so that all may be involved, e.g., by diabetes and malignancy. As a consequence, all individuals have undergo to laboratory investigations, as tumour biomarkers assessment, therefore spending uselessly NHS money, causing Psychological Jatrogenetic Terrorism, physician's energy and time loss. As a matter of fact, e.g., women can be involved by Oncological Terrain, even with or without precise location of inherited cancer real risk in a well defined breast quadrant ("ab posse ad esse non licet illatio", Kant, Kritik der reinigen Vernunft) (6). I think that because congenital functional mitochondrial cytopathology is overlooked - a "conditio sine qua non" of the most frequent and dangerous human disorders, including malignancies - current clinical researches are fundamentally biased. In other words, one does not consider the existence or assess the seriousness as well as the location of a mitochondrial cytopathy, I termed Congenital Acidosic Enzyme-Metabolic Histangiopathy, inherited by mother, conditio sine qua non of both Oncological Terrain and, consequently cancer "real risk" (3-5). In fact, both environmental risk factors and every drug, including oestrogens, suggested as a risk factor for breast cancer, "could" influence some human biological functions and/or bring about different disorders, such as cancers, exclusively in relation to both the presence and intensity of CAEMH in a well-defined biological system. For instance, despite either the well-known negative influence of radiation, and oral contraceptive use or the beneficial, positive effects of selective cyclooxygenase-2 (COX-2) inhibitors on breast oncogenesis (2) we have to consider the importance of the "genetic predispositions", i.e., Oncological Terrain, as far as the onset of a lot of disorders is concerned, including breast cancer. To summarize, we need at first, i.e., starting whatever screening or research, to investigate the presence and intensity of CAEMH in the tested population, i.e., in every, single patient, and soon thereafter assessing presence, intensity of the CAEMH-dependent, Oncological Terrain, and the precise location of cancer congenital real risk, both always develop on the basis of the above -mentioned congenital mitochondrial cytopathy. Really, without this alteration of psycho- neuro-endocrine-immunological system, oncogenesis is not possible, as allows me to state my long clinical experience with Quantum Biophysical Semeiotics, Single Patient Based Medicine theory is based on (7). Finally, these pathological conditions are characterized by microcirculatory remodelling, wherein a central role is played by newborn- pathological, type I, subtype a), i.e., oncological , Endoarteriolar Blocking Devices (2-6,15-17). The above mentioned advances in physical semeiotics will play a central role in the future pre-primary (Manuel's Story, Journal of Quantum Biophysical Semeiotics,http://www.sisbq.org/qbs-magazine.html) and primary prevention of common and dangerous disorders.
References
1)Gian Luigi Russo,Idolo Tedesco, Maria Russo, Angelo Cioppa, Maria Grazia Andreassi, and Eugenio Picano. Eur. Heart J. 2011 0:ehr263v1- ehr263; doi:10.1093/eurheartj/ehr263Cellular adaptive response to chronic radiation exposure in interventional cardiologists.
2)Stagnaro-Neri M., Stagnaro S. Introduzione alla Semeiotica Biofisica. Il Terreno Oncologico. Travel Factory, Roma, 2004. http://www.travelfactory.it
3) Stagnaro Sergio. There is another clinical, and overlooked tool, reliable in breast cancer prognosis evaluation http://www.biomedcentral.com/1471-2407/5/70/comments#204473 2005
4) Sergio Stagnaro Mitochondrial Bed-Side Evaluation: a new Way in the War against Cancer (21 December 2005). Cancer Cell International http://www.cancerci.com/content/5/1/34/comments#218502
5) Stagnaro S. Stagnaro S., Stagnaro-Neri M., La Melatonina nella Terapia del Terreno Oncologico e del "Reale Rischio" Oncologico. Travel Factory, Roma, 2004. http://www.travelfactory.it/semeiotica_biofisica_2.htm
6) Stagnaro-Neri M., Stagnaro S. Cancro della mammella: prevenzione primaria e diagnosi precoce con la percussione ascoltata. Gazz. Med. It. - Arch. Sc. Med. 152, 447, 1993
7) Stagnaro S., Stagnaro-Neri M., Single Patient Based Medicine.La Medicina Basata sul Singolo Paziente: Nuove Indicazioni della Melatonina. Travel Factory, Roma, 2005. http://www.travelfactory.it/libro_singlepatientbased.htm
8) Stagnaro Sergio. Clinical tool reliable in bedside early recognizing pancreas tumour, both benign and malignant. World Journal of Surgical Oncology 2005, 3:62 doi:10.1186/1477-7819-3-62, 2005
9) Stagnaro Sergio. Bed-Side Evaluating Breast Cancer Real Risk. World Journal of Surgical Oncology. 2005, 3:67 doi:10.1186/1477-7819-3-67. 2005 2005
10) Stagnaro Sergio. Mitochondrial Bed-Side Evaluation: a new Way in the War against Cancer (21 December 2005). Cancer Cell International http://www.cancerci.com/content/5/1/34/comments#218502 2005
11) Stagnaro Sergio. Cancer Risk Factors and Oncological Terrain. 2006. http://www.wjso.com/content/4/1/74/comments#247528 2006
12) Stagnaro Sergio. Without Oncological Terrain oncogenesis is not possible. CMAJ. 23 March 2007 http://www.cmaj.ca/cgi/eletters/176/5/646
13) Stagnaro Sergio. GPs , Biophysical Semeiotics, and bedside cancer diagnosis. 08 July 2007, International Seminar of Surgical Oncology, http://www.issoonline.com/content/4/1/11/comments#281539 , 2007
14) Stagnaro Sergio. Oncological Terrain and Inherited Oncological Real Risk: New Way in Malignancy Primary Prevention and early Diagnosis. International Seminars in Surgical Oncology, 2007. http://www.issoonline.com/content/4/1/25/comments#290565
15) Stagnaro Sergio. Bedside Biophysical-Semeiotic Diagnosis of Breast Cancer, since initial Stage. International Seminars in Surgical Oncology 2007, http://www.issoonline.com/content/4/1/21/comments
16) Stagnaro Sergio. Reale Rischio Semeiotico Biofisico. I Dispositivi Endoarteriolari di Blocco neoformati, patologici, tipo I, sottotipo a) oncologico, e b) aspecifico. Ediz. Travel Factory, www.travelfactory.it, Roma, 2009.
17) Caramel S., Stagnaro S. The role of mitochondria and mit-DNA in Oncogenesis. Quantum Biosystems 2010, 2, 221-248, http://www.quantumbiosystems.org/admin/files/QBS%202(1)%20250-281.pdf
Conflict of Interest:
None declared