





Abstract
Non-cardiac chest pain (NCCP) is considered a benign condition. We investigate case-fatality following an incident hospitalization for NCCP and determine whether previous psychiatric hospitalization is associated with short-term mortality.
This was a population-based retrospective cohort study of 159 888 patients discharged from hospital in Scotland (1991–2006) following a first NCCP hospitalization, using routinely collected morbidity and mortality data. All-cause and cardiovascular disease (CVD) mortality at 1 year following hospitalization was examined. A total of 3514 (4.4%) men and 3136 (3.9%) women with a first NCCP hospitalization had a psychiatric hospitalization in the 10 years preceding incident NCCP hospitalization. Those with a previous psychiatric hospitalization were younger and more socioeconomically deprived (SED). Overall, crude case fatality at 1 year was 4.4% in men and 3.7% in women. This was higher in patients with a previous psychiatric hospitalization compared with those without (overall: men 6.3 vs. 4.3%; women: 5.3 vs. 3.6%), in all age groups and all SED quintiles. Following adjustment (year of NCCP hospitalization, SED, co-morbid diabetes, and hypertension), the hazard of all-cause and CVD-specific death at 1 year was higher in men and women with a previous psychiatric hospitalization than without, with effect modification according to age group.
Non-cardiac chest pain is not an entirely benign condition. Individuals with a hospital discharge diagnosis of NCCP who have a previous psychiatric hospitalization have a greater risk of death, all-cause, and CVD-specific, at 1 year, than those without. A NCCP hospitalization is an opportunity to engage, and where appropriate, intervene to modify cardiovascular risk in this difficult-to-reach and high-risk group.
Introduction
Although the incidence of acute myocardial infarction (AMI) has fallen in recent years, there has been a substantial rise in hospitalizations for non-cardiac chest pain (NCCP), a diagnosis of exclusion.1 Between 1990 and 2000, the hospital-based incidence rate for NCCP in Scotland more than doubled.1 Despite reassurance from clinicians, patients with NCCP often experience persistent symptoms, impaired psychosocial functioning, and present repeatedly to the acute medical services.2 Non-cardiac chest pain is a significant, and increasing, burden on health care systems.1,2
Numerous studies have examined the bidirectional relationship between psychiatric disease and cardiovascular disease (CVD). Psychiatric morbidity is often experienced following an acute cardiac event.3 This may persist and indeed increase with subsequent events.4 Pre-existing psychiatric conditions including anxiety,5,6 depression,7,8 bipolar disorder,9 and schizophrenia10 are independent predictors of CVD mortality. This excess risk is mediated, in part, through modifiable cardiovascular risk factors (smoking, obesity, hypertension, and hyperlipidaemia) and the adverse effects of psychotropic medications,8,10–12 and compounded by the fact that compared with the general population, patients with psychiatric disease have less access to cardiovascular risk screening and preventative treatments.12
The relationship between psychiatric disorders and NCCP is less well characterized. Psychiatric disorders are more prevalent in patients diagnosed with NCCP compared with patients diagnosed with coronary heart disease (CHD).13 In addition, patients with NCCP often experience sustained psychiatric morbidity beyond that experienced by patients with CHD.14,15 This has led commentators to propose the use of psychological screening in patients presenting with NCCP. Early psychological intervention in a subgroup of ‘at risk’ patients following their first presentation with NCCP may reduce psychological morbidity and in turn improve quality of life and minimize health care seeking behaviour.13,16
Non-cardiac chest pain is considered a benign condition, associated with a low mortality rate.14,15 Yet, contemporary population-based studies describing outcomes in NCCP are lacking. To our knowledge, the relationship between psychiatric disorders and survival in patients with NCCP has not been investigated. We hypothesize that patients with NCCP are a heterogeneous group in whom the mortality experience differs according to the presence or absence of pre-existing psychiatric disease. The following data linkage study has two objectives: (i) investigate case fatality following a first hospitalization for NCCP; (2) examine the effect, if any, of a previous psychiatric hospitalization on short-term all-cause and CVD-specific mortality.
Methods
Data sources
Health care in Scotland is provided to all citizens, free at point of access, by the National Health Service (NHS). Virtually all elective and emergency hospital care is delivered by the NHS. Data on all discharges from NHS hospitals are collected by the Information and Statistics Division (ISD) of NHS Scotland using the Scottish Morbidity Record Scheme (SMR).17 In-patient and day case care delivered by general and acute specialties are captured in SMR01. The World Health Organization International Classification of Disease (ICD9 pre-1996, ICD10 post-1996) is used to code one principal (main condition) and up to five co-morbid discharge diagnoses identified from patient case records. In-patient and day case care delivered by mental health specialties are captured in SMR04. Up to four diagnoses, one main and three co-morbid diagnoses are ICD coded at both admission to and discharge from hospital. SMR01 and SMR04 are routinely linked to information held by the General Register Office for Scotland. For all deaths in Scotland, a death certificate is completed by a physician and returned to the Registrar General Office to be ICD coded. A sequence of diagnoses that led to an individual's death and co-morbid diagnoses which may have contributed to, but did not directly cause, death can be recorded on the certificate.
All hospitalizations in Scotland where NCCP (ICD9 786.5; ICD10 R072–R074) or ischaemic heart disease (IHD) (410–414; I20–I25) was coded as the principal (main condition) or as a secondary (co-morbid condition) diagnosis at discharge in SMR01, from 1981 to 2006, were identified. A first hospitalization for NCCP was defined as a hospitalization with a principal discharge diagnosis of NCCP and no previous hospitalization (principal or secondary diagnosis) for NCCP or IHD in the preceding 10 years. Co-morbid diagnoses of diabetes (250; E10–E14) and hypertension (401; I10–I13) were identified using principal and secondary diagnoses for any hospitalizations in the 5 years prior to the incident NCCP hospitalization. The SMR04 records of all patients with a first hospitalization for NCCP in the period 1991–2006 were examined. Using SMR04, patients who had been admitted to hospital under a mental health specialty within 10 years of incident NCCP hospitalization were identified. The underlying cause of death, that is the condition leading directly to death, was obtained for all deceased patients with an incident NCCP hospitalization from 1991 to 2006. Cause of death was considered in the following categories: CVD (900–459, I00–I99), cancer (140–239, C00–D48), respiratory disease (460–519, J00–J99), diseases of the digestive system (520–579, K00–K93), mental disorders and behavioural disorders including intentional self-harm (290–319, E950–E959, F00–F99, X60–X84), and a final group ‘other’ than encompassed all other causes of death not attributed to any of the aforementioned categories. Within the CVD grouping, cause of death was further characterized as CHD (410–414, I20–I25), cerebrovascular disease (430–438, I60–I69), and ‘other’ denoting all other forms of CVD.
Statistical analyses
Individuals were followed from the date of first hospitalization for NCCP to 31 December 2006. Analyses were conducted separately for men and women. Descriptive analyses were conducted first. Crude case fatality at 1 year following first NCCP hospitalization was then calculated. Exploratory analyses using Cox's proportional hazard modelling were carried out to determine whether specific psychiatric diagnoses were associated with excess mortality following adjustment for year of NCCP hospitalization, socioeconomic deprivation (SED), co-morbid diabetes, and co-morbid hypertension, in age and sex-specific models. Two broad categories of psychiatric diagnoses were considered: (i) affective disorders, schizophrenia, and/or schizotypal disorders (295, 296; F20–F39) and (ii) all other psychiatric disorders. The hazard ratios for total mortality at 1 year were of a similar magnitude irrespective of the definition of psychiatric illness used, both resembling those for ‘any’ psychiatric diagnosis. There were too few CVD deaths in men and women to facilitate analyses. We therefore examined the association between mortality and ‘any’ psychiatric diagnosis using Cox's proportional hazard modelling adjusting for year of first NCCP hospitalization, SED, as measured in quintiles by the Carstairs Morris Index of Multiple Deprivation based on 1991 census,18 and co-morbid diagnoses of diabetes and hypertension. The proportional hazards assumption was met for each model. Two-sided testing was performed with a significance level of 0.05 used throughout. All analyses were carried out using STATA (Version 11, Stata Corp).
Results
Patient characteristics
Between 1991 and 2006, there were 159 888 first hospitalizations for NCCP in Scotland; 79 176 (49.5%) were in men. The absolute number of first hospitalizations for NCCP in men increased from 3193 per year in 1991 to 6501 in 2006. The corresponding values in women were 2766 and 7237. In total, 4.4% of men and 3.9% of women had been admitted to hospital under a mental health specialty in the 10 years prior to the first hospitalization for NCCP. This was invariant over time in both men (P= 0.803) and women (P= 0.506). The median time from psychiatric hospitalization to NCCP hospitalization was 994 (IQR 307–2113) days in men and 1079 (322–2190) days in women.
Patients with a previous psychiatric hospitalization were approximately 3 years younger than those without (Table 1); the mean age in men was 48.3 (SD 13.4) years compared with 51.2 (15.5) years and in women 51.1 (15.9) years compared with 54.0 (16.8) years (P< 0.01 both). Men and women with a previous psychiatric hospitalization were more SED than those without a previous psychiatric hospitalization (P< 0.01 both). Approximately one-third of individuals with a previous psychiatric hospitalization were in the most SED group compared with a quarter of men and women without.
Baseline characteristics of men and women with a first hospitalization for non-cardiac chest pain in Scotland, 1991–2006
| Men | P-value | Women | P-value | |||
|---|---|---|---|---|---|---|
| Psychiatric hospitalization | Psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Total number, (%) | 3514 (4.4) | 75 662 (95.6) | 3136 (3.9) | 77 576 (96.1) | ||
| Mean age, years (SD) | 48.3 (13.4) | 51.2 (15.5) | <0.01 | 51.1 (15.9) | 54.0 (16.8) | <0.01 |
| Age group in years, n (%) | ||||||
| ≤40 | 912 (26.0) | 17 111 (22.6) | <0.01 | 724 (23.1) | 15 071 (19.4) | <0.01 |
| 40–49 | 1120 (31.9) | 19 213 (25.4) | 908 (29.0) | 16 380 (21.1) | ||
| 50–59 | 822 (23.4) | 17 184 (22.7) | 646 (20.6) | 17 687 (22.8) | ||
| ≥60 | 660 (18.8) | 22 154 (29.3) | 858 (27.4) | 28 438 (36.7) | ||
| Socioeconomic deprivation (quintiles), n (%) | ||||||
| 1 (least deprived) | 372 (10.6) | 12 003 (15.9) | <0.01 | 363 (11.5) | 12 344 (15.9) | <0.01 |
| 2 | 482 (13.8) | 13 311 (17.6) | 449 (14.3) | 13 679 (17.6) | ||
| 3 | 592 (16.8) | 14 644 (19.4) | 561 (17.9) | 14 775 (19.0) | ||
| 4 | 828 (23.5) | 15 864 (21.0) | 731 (23.3) | 16 138 (20.8) | ||
| 5 (most deprived) | 1240 (35.3) | 19 840 (26.2) | 1032 (32.9) | 20 640 (26.6) | ||
| Men | P-value | Women | P-value | |||
|---|---|---|---|---|---|---|
| Psychiatric hospitalization | Psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Total number, (%) | 3514 (4.4) | 75 662 (95.6) | 3136 (3.9) | 77 576 (96.1) | ||
| Mean age, years (SD) | 48.3 (13.4) | 51.2 (15.5) | <0.01 | 51.1 (15.9) | 54.0 (16.8) | <0.01 |
| Age group in years, n (%) | ||||||
| ≤40 | 912 (26.0) | 17 111 (22.6) | <0.01 | 724 (23.1) | 15 071 (19.4) | <0.01 |
| 40–49 | 1120 (31.9) | 19 213 (25.4) | 908 (29.0) | 16 380 (21.1) | ||
| 50–59 | 822 (23.4) | 17 184 (22.7) | 646 (20.6) | 17 687 (22.8) | ||
| ≥60 | 660 (18.8) | 22 154 (29.3) | 858 (27.4) | 28 438 (36.7) | ||
| Socioeconomic deprivation (quintiles), n (%) | ||||||
| 1 (least deprived) | 372 (10.6) | 12 003 (15.9) | <0.01 | 363 (11.5) | 12 344 (15.9) | <0.01 |
| 2 | 482 (13.8) | 13 311 (17.6) | 449 (14.3) | 13 679 (17.6) | ||
| 3 | 592 (16.8) | 14 644 (19.4) | 561 (17.9) | 14 775 (19.0) | ||
| 4 | 828 (23.5) | 15 864 (21.0) | 731 (23.3) | 16 138 (20.8) | ||
| 5 (most deprived) | 1240 (35.3) | 19 840 (26.2) | 1032 (32.9) | 20 640 (26.6) | ||
Baseline characteristics of men and women with a first hospitalization for non-cardiac chest pain in Scotland, 1991–2006
| Men | P-value | Women | P-value | |||
|---|---|---|---|---|---|---|
| Psychiatric hospitalization | Psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Total number, (%) | 3514 (4.4) | 75 662 (95.6) | 3136 (3.9) | 77 576 (96.1) | ||
| Mean age, years (SD) | 48.3 (13.4) | 51.2 (15.5) | <0.01 | 51.1 (15.9) | 54.0 (16.8) | <0.01 |
| Age group in years, n (%) | ||||||
| ≤40 | 912 (26.0) | 17 111 (22.6) | <0.01 | 724 (23.1) | 15 071 (19.4) | <0.01 |
| 40–49 | 1120 (31.9) | 19 213 (25.4) | 908 (29.0) | 16 380 (21.1) | ||
| 50–59 | 822 (23.4) | 17 184 (22.7) | 646 (20.6) | 17 687 (22.8) | ||
| ≥60 | 660 (18.8) | 22 154 (29.3) | 858 (27.4) | 28 438 (36.7) | ||
| Socioeconomic deprivation (quintiles), n (%) | ||||||
| 1 (least deprived) | 372 (10.6) | 12 003 (15.9) | <0.01 | 363 (11.5) | 12 344 (15.9) | <0.01 |
| 2 | 482 (13.8) | 13 311 (17.6) | 449 (14.3) | 13 679 (17.6) | ||
| 3 | 592 (16.8) | 14 644 (19.4) | 561 (17.9) | 14 775 (19.0) | ||
| 4 | 828 (23.5) | 15 864 (21.0) | 731 (23.3) | 16 138 (20.8) | ||
| 5 (most deprived) | 1240 (35.3) | 19 840 (26.2) | 1032 (32.9) | 20 640 (26.6) | ||
| Men | P-value | Women | P-value | |||
|---|---|---|---|---|---|---|
| Psychiatric hospitalization | Psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Total number, (%) | 3514 (4.4) | 75 662 (95.6) | 3136 (3.9) | 77 576 (96.1) | ||
| Mean age, years (SD) | 48.3 (13.4) | 51.2 (15.5) | <0.01 | 51.1 (15.9) | 54.0 (16.8) | <0.01 |
| Age group in years, n (%) | ||||||
| ≤40 | 912 (26.0) | 17 111 (22.6) | <0.01 | 724 (23.1) | 15 071 (19.4) | <0.01 |
| 40–49 | 1120 (31.9) | 19 213 (25.4) | 908 (29.0) | 16 380 (21.1) | ||
| 50–59 | 822 (23.4) | 17 184 (22.7) | 646 (20.6) | 17 687 (22.8) | ||
| ≥60 | 660 (18.8) | 22 154 (29.3) | 858 (27.4) | 28 438 (36.7) | ||
| Socioeconomic deprivation (quintiles), n (%) | ||||||
| 1 (least deprived) | 372 (10.6) | 12 003 (15.9) | <0.01 | 363 (11.5) | 12 344 (15.9) | <0.01 |
| 2 | 482 (13.8) | 13 311 (17.6) | 449 (14.3) | 13 679 (17.6) | ||
| 3 | 592 (16.8) | 14 644 (19.4) | 561 (17.9) | 14 775 (19.0) | ||
| 4 | 828 (23.5) | 15 864 (21.0) | 731 (23.3) | 16 138 (20.8) | ||
| 5 (most deprived) | 1240 (35.3) | 19 840 (26.2) | 1032 (32.9) | 20 640 (26.6) | ||
Overall, the prevalence of diabetes as a co-morbid diagnosis was 1.9% in men and women. This varied according to previous psychiatric hospitalization such that both men (2.5 vs. 1.8%, P< 0.01) and women (3.6 vs. 1.9%, P< 0.01) with a previous psychiatric hospitalization were more likely to have a co-morbid diagnosis of diabetes than those without. A similar pattern was observed for co-morbid hypertension (men 3.8 vs. 2.9%, P< 0.01; women 5.0 vs. 3.7%, P< 0.01).
Crude case fatality
Overall crude case fatality at 1 year was 4.4% in men and 3.7% in women (Table 2). This increased with age, from 0.6% (0.6%) in men (women) aged 40 years or under to 11.4% (8.3%) in men (women) aged 60 years or over. Crude case fatality was higher in men and women with a previous psychiatric hospitalization than those without; overall, 6.3 vs. 4.3% in men and 5.4 vs. 3.6% in women. This was true of all age groups and all SED quintiles. Proximity of psychiatric hospitalization to incident NCCP hospitalization appeared to be associated with greater crude case fatality in men and women. For example, all-cause case fatality in men with a previous psychiatric hospitalization was 9.6, 5.8, and 3.8%, respectively, in the time periods 0–1 year, 1–5 years, and 5–10 years from psychiatric hospitalization to NCCP hospitalization. Corresponding values for women were 8.7, 4.9, and 3.6%.
Crude case fatality 1 year following first hospitalization for non-cardiac chest pain in men and women, according to psychiatric hospitalization
| All patients | Men | All patients | Women | |||
|---|---|---|---|---|---|---|
| Psychiatric hospitalization | Psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Total, % (n) | 4.4 (3508) | 6.3 (220) | 4.3 (3288) | 3.7 (2995) | 5.4 (168) | 3.6 (2827) |
| Age group in years, % (n) | ||||||
| ≤40 | 0.6 (112) | 2.1 (19) | 0.6 (93) | 0.6 (94) | 1.7 (12) | 0.5 (82) |
| 40–49 | 1.3 (254) | 3.8 (43) | 1.1 (211) | 0.9 (161) | 1.9 (17) | 0.9 (144) |
| 50–59 | 3.0 (547) | 6.8 (56) | 2.9 (491) | 1.7 (305) | 2.9 (19) | 1.6 (286) |
| ≥60 | 11.4 (2595) | 15.4 (102) | 11.3 (2493) | 8.3 (2435) | 13.9 (120) | 8.1 (2315) |
| Socioeconomic deprivation quintile, % (n) | ||||||
| 1 (least deprived) | 4.1 (510) | 8.3 (31) | 4.0 (479) | 3.5 (444) | 6.1 (23) | 3.4 (421) |
| 2 | 4.5 (623) | 5.6 (27) | 4.5 (596) | 3.6 (508) | 4.9 (22) | 3.6 (486) |
| 3 | 4.3 (649) | 5.7 (34) | 4.2 (615) | 3.6 (556) | 5.3 (30) | 3.6 (526) |
| 4 | 4.6 (763) | 6.2 (51) | 4.5 (712) | 3.9 (655) | 6.2 (45) | 3.8 (610) |
| 5 (most deprived) | 4.6 (963) | 6.2 (77) | 4.5 (886) | 3.8 (832) | 4.7 (48) | 3.8 (784) |
| All patients | Men | All patients | Women | |||
|---|---|---|---|---|---|---|
| Psychiatric hospitalization | Psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Total, % (n) | 4.4 (3508) | 6.3 (220) | 4.3 (3288) | 3.7 (2995) | 5.4 (168) | 3.6 (2827) |
| Age group in years, % (n) | ||||||
| ≤40 | 0.6 (112) | 2.1 (19) | 0.6 (93) | 0.6 (94) | 1.7 (12) | 0.5 (82) |
| 40–49 | 1.3 (254) | 3.8 (43) | 1.1 (211) | 0.9 (161) | 1.9 (17) | 0.9 (144) |
| 50–59 | 3.0 (547) | 6.8 (56) | 2.9 (491) | 1.7 (305) | 2.9 (19) | 1.6 (286) |
| ≥60 | 11.4 (2595) | 15.4 (102) | 11.3 (2493) | 8.3 (2435) | 13.9 (120) | 8.1 (2315) |
| Socioeconomic deprivation quintile, % (n) | ||||||
| 1 (least deprived) | 4.1 (510) | 8.3 (31) | 4.0 (479) | 3.5 (444) | 6.1 (23) | 3.4 (421) |
| 2 | 4.5 (623) | 5.6 (27) | 4.5 (596) | 3.6 (508) | 4.9 (22) | 3.6 (486) |
| 3 | 4.3 (649) | 5.7 (34) | 4.2 (615) | 3.6 (556) | 5.3 (30) | 3.6 (526) |
| 4 | 4.6 (763) | 6.2 (51) | 4.5 (712) | 3.9 (655) | 6.2 (45) | 3.8 (610) |
| 5 (most deprived) | 4.6 (963) | 6.2 (77) | 4.5 (886) | 3.8 (832) | 4.7 (48) | 3.8 (784) |
Crude case fatality 1 year following first hospitalization for non-cardiac chest pain in men and women, according to psychiatric hospitalization
| All patients | Men | All patients | Women | |||
|---|---|---|---|---|---|---|
| Psychiatric hospitalization | Psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Total, % (n) | 4.4 (3508) | 6.3 (220) | 4.3 (3288) | 3.7 (2995) | 5.4 (168) | 3.6 (2827) |
| Age group in years, % (n) | ||||||
| ≤40 | 0.6 (112) | 2.1 (19) | 0.6 (93) | 0.6 (94) | 1.7 (12) | 0.5 (82) |
| 40–49 | 1.3 (254) | 3.8 (43) | 1.1 (211) | 0.9 (161) | 1.9 (17) | 0.9 (144) |
| 50–59 | 3.0 (547) | 6.8 (56) | 2.9 (491) | 1.7 (305) | 2.9 (19) | 1.6 (286) |
| ≥60 | 11.4 (2595) | 15.4 (102) | 11.3 (2493) | 8.3 (2435) | 13.9 (120) | 8.1 (2315) |
| Socioeconomic deprivation quintile, % (n) | ||||||
| 1 (least deprived) | 4.1 (510) | 8.3 (31) | 4.0 (479) | 3.5 (444) | 6.1 (23) | 3.4 (421) |
| 2 | 4.5 (623) | 5.6 (27) | 4.5 (596) | 3.6 (508) | 4.9 (22) | 3.6 (486) |
| 3 | 4.3 (649) | 5.7 (34) | 4.2 (615) | 3.6 (556) | 5.3 (30) | 3.6 (526) |
| 4 | 4.6 (763) | 6.2 (51) | 4.5 (712) | 3.9 (655) | 6.2 (45) | 3.8 (610) |
| 5 (most deprived) | 4.6 (963) | 6.2 (77) | 4.5 (886) | 3.8 (832) | 4.7 (48) | 3.8 (784) |
| All patients | Men | All patients | Women | |||
|---|---|---|---|---|---|---|
| Psychiatric hospitalization | Psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Total, % (n) | 4.4 (3508) | 6.3 (220) | 4.3 (3288) | 3.7 (2995) | 5.4 (168) | 3.6 (2827) |
| Age group in years, % (n) | ||||||
| ≤40 | 0.6 (112) | 2.1 (19) | 0.6 (93) | 0.6 (94) | 1.7 (12) | 0.5 (82) |
| 40–49 | 1.3 (254) | 3.8 (43) | 1.1 (211) | 0.9 (161) | 1.9 (17) | 0.9 (144) |
| 50–59 | 3.0 (547) | 6.8 (56) | 2.9 (491) | 1.7 (305) | 2.9 (19) | 1.6 (286) |
| ≥60 | 11.4 (2595) | 15.4 (102) | 11.3 (2493) | 8.3 (2435) | 13.9 (120) | 8.1 (2315) |
| Socioeconomic deprivation quintile, % (n) | ||||||
| 1 (least deprived) | 4.1 (510) | 8.3 (31) | 4.0 (479) | 3.5 (444) | 6.1 (23) | 3.4 (421) |
| 2 | 4.5 (623) | 5.6 (27) | 4.5 (596) | 3.6 (508) | 4.9 (22) | 3.6 (486) |
| 3 | 4.3 (649) | 5.7 (34) | 4.2 (615) | 3.6 (556) | 5.3 (30) | 3.6 (526) |
| 4 | 4.6 (763) | 6.2 (51) | 4.5 (712) | 3.9 (655) | 6.2 (45) | 3.8 (610) |
| 5 (most deprived) | 4.6 (963) | 6.2 (77) | 4.5 (886) | 3.8 (832) | 4.7 (48) | 3.8 (784) |
Cause of death at 1 year
Cause of death at 1 year following first hospitalization for NCCP is outlined in Table 3. In both men and women with a previous psychiatric hospitalization, the most frequent cause of death was CVD accounting for 28.2 and 44.1% of all deaths, respectively. In men and women without a history of previous psychiatric hospitalization, the most common cause of death was cancer, accounting for 41.5 and 38.0% of deaths, respectively.
Cause of death 1 year following first hospitalization for non-cardiac chest pain in men and women, according to psychiatric hospitalization
| Cause of death, n (%) | Men | P-value | Women | P-value | ||
|---|---|---|---|---|---|---|
| Previous psychiatric hospitalization | Previous psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Cardiovascular disease | 62 (28.2) | 1121 (34.1) | <0.01 | 74 (44.1) | 1054 (37.3) | <0.01 |
| Coronary heart disease | 40 (64.5) | 741 (66.1) | 39 (52.7) | 608 (57.7) | ||
| Cerebrovascular disease | 11 (17.7) | 168 (15.0) | 21 (28.4) | 202 (19.2) | ||
| Other | 11 (17.7) | 212 (18.9) | 14 (18.9) | 244 (23.2) | ||
| Respiratory disease | 29 (13.2) | 319 (9.7) | 33 (19.6) | 324 (11.5) | ||
| Cancer | 37 (16.8) | 1365 (41.5) | 23 (13.7) | 1073 (38.0) | ||
| Digestive disease | 32 (14.6) | 158 (4.8) | 9 (5.4) | 131 (4.6) | ||
| Mental disorders and intentional self-harm | 38 (17.3) | 76 (2.3) | 11 (6.6) | 36 (1.3) | ||
| Other | 22 (10.0) | 249 (7.6) | 18 (10.7) | 209 (7.4) | ||
| Cause of death, n (%) | Men | P-value | Women | P-value | ||
|---|---|---|---|---|---|---|
| Previous psychiatric hospitalization | Previous psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Cardiovascular disease | 62 (28.2) | 1121 (34.1) | <0.01 | 74 (44.1) | 1054 (37.3) | <0.01 |
| Coronary heart disease | 40 (64.5) | 741 (66.1) | 39 (52.7) | 608 (57.7) | ||
| Cerebrovascular disease | 11 (17.7) | 168 (15.0) | 21 (28.4) | 202 (19.2) | ||
| Other | 11 (17.7) | 212 (18.9) | 14 (18.9) | 244 (23.2) | ||
| Respiratory disease | 29 (13.2) | 319 (9.7) | 33 (19.6) | 324 (11.5) | ||
| Cancer | 37 (16.8) | 1365 (41.5) | 23 (13.7) | 1073 (38.0) | ||
| Digestive disease | 32 (14.6) | 158 (4.8) | 9 (5.4) | 131 (4.6) | ||
| Mental disorders and intentional self-harm | 38 (17.3) | 76 (2.3) | 11 (6.6) | 36 (1.3) | ||
| Other | 22 (10.0) | 249 (7.6) | 18 (10.7) | 209 (7.4) | ||
Cause of death 1 year following first hospitalization for non-cardiac chest pain in men and women, according to psychiatric hospitalization
| Cause of death, n (%) | Men | P-value | Women | P-value | ||
|---|---|---|---|---|---|---|
| Previous psychiatric hospitalization | Previous psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Cardiovascular disease | 62 (28.2) | 1121 (34.1) | <0.01 | 74 (44.1) | 1054 (37.3) | <0.01 |
| Coronary heart disease | 40 (64.5) | 741 (66.1) | 39 (52.7) | 608 (57.7) | ||
| Cerebrovascular disease | 11 (17.7) | 168 (15.0) | 21 (28.4) | 202 (19.2) | ||
| Other | 11 (17.7) | 212 (18.9) | 14 (18.9) | 244 (23.2) | ||
| Respiratory disease | 29 (13.2) | 319 (9.7) | 33 (19.6) | 324 (11.5) | ||
| Cancer | 37 (16.8) | 1365 (41.5) | 23 (13.7) | 1073 (38.0) | ||
| Digestive disease | 32 (14.6) | 158 (4.8) | 9 (5.4) | 131 (4.6) | ||
| Mental disorders and intentional self-harm | 38 (17.3) | 76 (2.3) | 11 (6.6) | 36 (1.3) | ||
| Other | 22 (10.0) | 249 (7.6) | 18 (10.7) | 209 (7.4) | ||
| Cause of death, n (%) | Men | P-value | Women | P-value | ||
|---|---|---|---|---|---|---|
| Previous psychiatric hospitalization | Previous psychiatric hospitalization | |||||
| Yes | No | Yes | No | |||
| Cardiovascular disease | 62 (28.2) | 1121 (34.1) | <0.01 | 74 (44.1) | 1054 (37.3) | <0.01 |
| Coronary heart disease | 40 (64.5) | 741 (66.1) | 39 (52.7) | 608 (57.7) | ||
| Cerebrovascular disease | 11 (17.7) | 168 (15.0) | 21 (28.4) | 202 (19.2) | ||
| Other | 11 (17.7) | 212 (18.9) | 14 (18.9) | 244 (23.2) | ||
| Respiratory disease | 29 (13.2) | 319 (9.7) | 33 (19.6) | 324 (11.5) | ||
| Cancer | 37 (16.8) | 1365 (41.5) | 23 (13.7) | 1073 (38.0) | ||
| Digestive disease | 32 (14.6) | 158 (4.8) | 9 (5.4) | 131 (4.6) | ||
| Mental disorders and intentional self-harm | 38 (17.3) | 76 (2.3) | 11 (6.6) | 36 (1.3) | ||
| Other | 22 (10.0) | 249 (7.6) | 18 (10.7) | 209 (7.4) | ||
Adjusted all-cause mortality
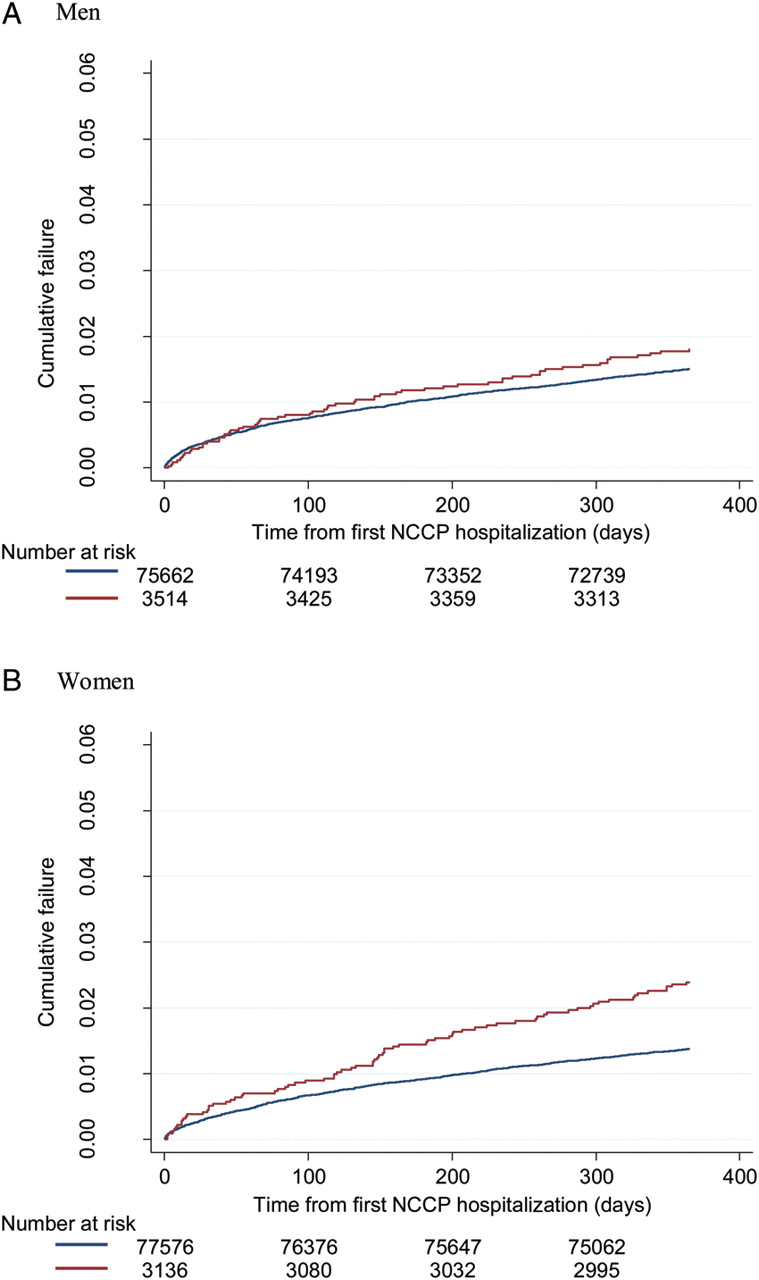
Kaplan–Meier curves for all-cause death at 1 year in men and women according to history of previous psychiatric hospitalization are shown in Figure 1. Age- and sex-specific hazards of death at 1 year in patients with, compared to without, a previous psychiatric hospitalization are shown in Table 4. A previous psychiatric hospitalization was associated with an elevated risk of all-cause mortality in all groups. The relative risk was greatest in the youngest age group, in men HR 3.75 (95% CI 2.28–6.15), and fell with age, although an excess risk persisted in the elderly, HR 1.39 (1.14–1.69). Similar trends are reported for women.
Age- and sex-specific hazard ratios for death, all-cause, and cardiovascular disease specific, at 1 year following first hospitalization with non-cardiac chest pain in patients with a previous psychiatric hospitalization compared with those without
| Age group, years | Hazard ratios (95% CI)a | |||
|---|---|---|---|---|
| All-cause mortality | CVD mortality | |||
| Men | Women | Men | Women | |
| ≤40 | 3.71 (2.26–6.09) | 2.94 (1.60–5.41) | 2.81 (0.83–9.56) | 3.71 (1.06–12.92) |
| 40–49 | 3.40 (2.44–4.73) | 2.05 (1.23–3.39) | 2.66 (1.36–5.20) | 2.77 (0.96–7.99) |
| 50–59 | 2.24 (1.70–2.96) | 1.62 (1.01–2.58) | 1.40 (0.74–2.67) | 2.16 (0.93–5.06) |
| ≥60 | 1.37 (1.12–1.67) | 1.70 (1.42–2.05) | 1.43 (1.04–1.97) | 2.08 (1.61–2.69) |
| Age group, years | Hazard ratios (95% CI)a | |||
|---|---|---|---|---|
| All-cause mortality | CVD mortality | |||
| Men | Women | Men | Women | |
| ≤40 | 3.71 (2.26–6.09) | 2.94 (1.60–5.41) | 2.81 (0.83–9.56) | 3.71 (1.06–12.92) |
| 40–49 | 3.40 (2.44–4.73) | 2.05 (1.23–3.39) | 2.66 (1.36–5.20) | 2.77 (0.96–7.99) |
| 50–59 | 2.24 (1.70–2.96) | 1.62 (1.01–2.58) | 1.40 (0.74–2.67) | 2.16 (0.93–5.06) |
| ≥60 | 1.37 (1.12–1.67) | 1.70 (1.42–2.05) | 1.43 (1.04–1.97) | 2.08 (1.61–2.69) |
aAdjusted for year of first NCCP hospitalization, SED quintile, co-morbid diabetes, and hypertension.
Age- and sex-specific hazard ratios for death, all-cause, and cardiovascular disease specific, at 1 year following first hospitalization with non-cardiac chest pain in patients with a previous psychiatric hospitalization compared with those without
| Age group, years | Hazard ratios (95% CI)a | |||
|---|---|---|---|---|
| All-cause mortality | CVD mortality | |||
| Men | Women | Men | Women | |
| ≤40 | 3.71 (2.26–6.09) | 2.94 (1.60–5.41) | 2.81 (0.83–9.56) | 3.71 (1.06–12.92) |
| 40–49 | 3.40 (2.44–4.73) | 2.05 (1.23–3.39) | 2.66 (1.36–5.20) | 2.77 (0.96–7.99) |
| 50–59 | 2.24 (1.70–2.96) | 1.62 (1.01–2.58) | 1.40 (0.74–2.67) | 2.16 (0.93–5.06) |
| ≥60 | 1.37 (1.12–1.67) | 1.70 (1.42–2.05) | 1.43 (1.04–1.97) | 2.08 (1.61–2.69) |
| Age group, years | Hazard ratios (95% CI)a | |||
|---|---|---|---|---|
| All-cause mortality | CVD mortality | |||
| Men | Women | Men | Women | |
| ≤40 | 3.71 (2.26–6.09) | 2.94 (1.60–5.41) | 2.81 (0.83–9.56) | 3.71 (1.06–12.92) |
| 40–49 | 3.40 (2.44–4.73) | 2.05 (1.23–3.39) | 2.66 (1.36–5.20) | 2.77 (0.96–7.99) |
| 50–59 | 2.24 (1.70–2.96) | 1.62 (1.01–2.58) | 1.40 (0.74–2.67) | 2.16 (0.93–5.06) |
| ≥60 | 1.37 (1.12–1.67) | 1.70 (1.42–2.05) | 1.43 (1.04–1.97) | 2.08 (1.61–2.69) |
aAdjusted for year of first NCCP hospitalization, SED quintile, co-morbid diabetes, and hypertension.
Kaplan–Meier cumulative failure curve for death (all–cause) at 1 year in (A) men and (B) women with a first hospitalization for non-cardiac chest pain according to history of previous psychiatric hospitalization. (Red line) Previous psychiatric hospitalization. (Blue line) No previous psychiatric hospitalization.
Adjusted cardiovascular disease-specific mortality
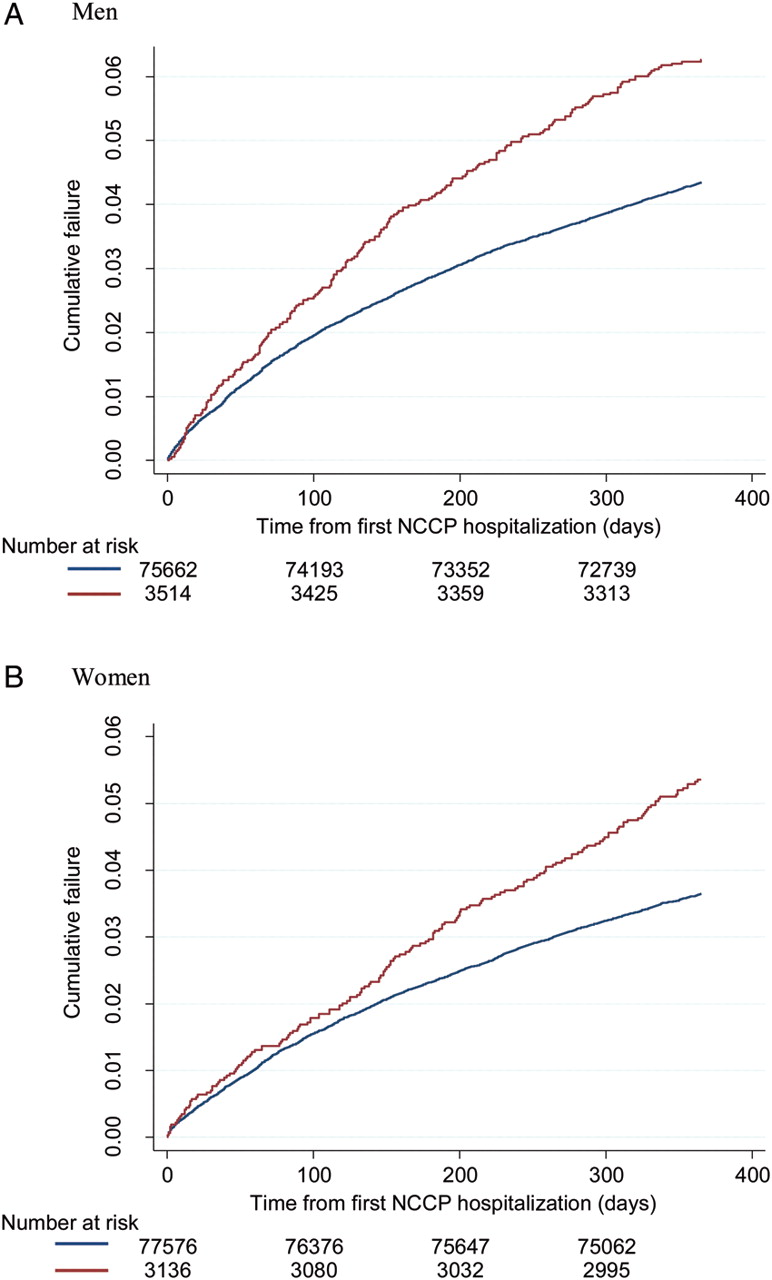
Kaplan–Meier curves for CVD death at 1 year in men and women according to history of previous psychiatric hospitalization are shown in Figure 2. A previous psychiatric hospitalization was associated with an elevated risk of CVD death in all groups (Table 4). This relative risk was highest in the youngest group [HR 2.94 (0.86–10.04) in men and 4.41 (1.26–15.40) in women] and decreased with advancing age [HR 1.45 (1.05–2.00) in men and 2.12 (1.64–2.75) in women aged 60 years and over].
Kaplan–Meier cumulative failure curve for cardiovascular disease death at 1 year in (A) men and (B) women with a first hospitalization for non-cardiac chest pain according to history of previous psychiatric hospitalization. (Red line) Previous psychiatric hospitalization. (Blue line) No previous psychiatric hospitalization.
Discussion
Summary of main findings
In our study, NCCP was not a benign diagnosis; short-term case fatality following a first hospitalization for NCCP in individuals otherwise free from IHD was high. Previous psychiatric hospitalization was associated with all-cause and CVD-specific mortality in patients hospitalized for NCCP. These effects were independent of SED. However, age was an effect modifier: that is, the relative risk of total and CVD-specific mortality associated with psychiatric illness was greatest in men and women in the youngest age groups. To our knowledge, this is the first study to examine the association between previous psychiatric hospitalization and mortality in patients hospitalized for NCCP.
Relevance of findings
Previous studies have suggested NCCP is a benign condition that, while associated with a high risk of rehospitalization for NCCP and ongoing symptomatology, is not associated with excess mortality.14,15 Overall crude case fatality at 1 year in our study was 4.4% in men and 3.7% in women with a strong age gradient, increasing from less than 1% in men and women aged 40 years or younger, to 11.4% in men and 8.3% in women aged 60 years and over.
A small number of studies have reported high short-term mortality in patients with NCCP. In a prospective cohort study of consecutive patients admitted to the emergency department with chest pain in a tertiary teaching hospital in Australia, Eslick and Talley19 reported comparable rates of cardiac death at 2 years in patients with a cardiac diagnosis and those with NCCP (cardiac case-fatality rates were 11 vs. 5.5%, respectively, P= 0.16). Advancing age independently predicted mortality. In a large multicentre study of rapid access chest pain clinics (RACPC) in England, Sekhri et al.20 followed 8762 consecutive patients from assessment for a median of 2.5 years reporting a composite primary end-point of CHD death, non-fatal AMI, or hospitalization for unstable angina. The cumulative incidence of primary end-points was lower for patients with NCCP than those diagnosed with angina at 1 year [0.83% (0.63–1.08) vs. 8.62% (7.56–9.83)] and 3-year follow-up [2.73% (2.29–3.25) vs. 16.52% (14.88–18.32)]. However, one-third of all primary end-points occurred in patients diagnosed with NCCP. Individuals with diabetes, of South Asian origin, and with an abnormal ECG were identified as being at excess risk. The authors considered that this group was most likely misdiagnosed at initial assessment; young age, atypical symptoms, and a normal resting ECG contributing to difficulties reaching a diagnosis. Ruigomez et al.21 carried out a nested case–control study using the UK General Practice Research Database (UKGPRD) to assess morbidity and mortality in 3028 men and women without established IHD presenting to primary care with a first consultation for NCCP. At 1-year follow-up, patients with NCCP were significantly more likely than age- and sex-matched controls to receive an incident diagnosis of IHD [HR 18.3 (11.6–28.6)] or die [HR 2.3 (1.3–4.1)]. Excess deaths were largely attributable to IHD and cancer. These studies, in different patient populations and health care settings, suggest a proportion of patients diagnosed with NCCP actually have undiagnosed IHD. Current approaches to the assessment of patients with NCCP may lead to the diagnosis of IHD being missed in specific patient populations.
To our knowledge, this is the first study to examine the association between prior psychiatric hospitalization and survival in patients hospitalized with NCCP. Case fatality was significantly higher in those with a psychiatric disorder than without. The crude case fatality we observed in men with NCCP and a previous psychiatric hospitalization was comparable with that reported in men presenting with an incident hospitalization for AMI or angina in Scotland (6.3 vs. 6.4% or 6.5%; in women, the corresponding figures were 5.4 vs. 8.9% or 6.4%).22 The implications are three-fold. First, our data suggest that previous psychiatric hospitalization should be considered in the risk stratification of patients presenting with NCCP. Patients with severe mental illness have been shown to have a greater risk of cardiac death than age-matched population controls, with the risk being greatest in the youngest age groups.5 While psychiatric disease is associated with adverse cardiovascular risk profiles, it is not known whether this would fully account for the excess risk we observed. Psychiatric disease has been shown to be an independent risk factor for metabolic disturbance for example.23 It is therefore important that psychiatric disease, such as SED, is considered in cardiovascular risk assessment.
Secondly, the application of standard diagnostic technologies in the investigation of suspect cardiac chest pain in patients with psychiatric disorders may not be effective. The study by Sekhri et al.20 noted that misdiagnosis at RACPC was more likely in young patients with atypical symptoms. We found the relative risk of excess mortality was greatest in young men and women. While we do not have information on the reporting of symptoms, it is conceivable that active psychiatric disease could impair a patients' ability to effectively communicate their symptoms. Moreover, we do not know how, if at all, a health care professional's assessment and management might be influenced by the knowledge that a patient has had an episode of severe mental illness. Research to increase the diagnostic sensitivity of non-invasive investigations to exclude cardiac disease in all patients with NCCP, and specific subgroups at excess risk, is welcomed.
Finally, having identified and engaged with a group of patients at excess risk, a window of opportunity exists to deliver appropriately tailored risk reduction interventions. Patients with psychiatric disease may be at excess risk from CVD for a number of reasons.12 This vulnerable group is often difficult to reach and may experience poor-quality medical care.24 While psychiatrists often have the greatest access to this patient group, the care of patients with psychiatric disorders and physical illness should be shared with physicians from primary care and specialists in secondary care.12 Patients with psychiatric disease lead less favourable lifestyles (heavy smoking, excessive alcohol use, poor diet, and sedentary behaviour) than the general population and many psychotropic medications have both cardiovascular and metabolic side effects.8,10–12 Opportunities to engage patients with severe mental illness in cardiovascular risk screening are missed.24 Cardiovascular risk scores such as Framingham may underestimate risk, particularly in young SED patients.11,12 Among patients with severe mental illness in whom modifiable cardiovascular risk factors have been identified, rates of treatment for hypertension, hyperlipidaemia, and diabetes are low.25 Early identification and intervention to modify cardiovascular risk factors in this population may reduce subsequent events and should be aggressively pursued, a view supported by a recent joint position statement issued by the European Psychiatric Association and European Society of Cardiology.12 A first hospitalization for NCCP represents an opportunity to comprehensively assess cardiovascular risk and engage this vulnerable population in the management of that risk. In our study, proximity of NCCP hospitalization to psychiatric hospitalization was associated with higher crude case fatality. The optimal time to asses and modify cardiovascular risk may therefore be at initial psychiatric hospitalization, with on-going cardiovascular risk factor monitoring being an integral part of routine care in this population. To do this effectively, we must first understand the factors that independently contribute to excess risk in this population and develop risk scores that accurately assess risk and predict outcome.
Strengths and limitations
There are number of limitations to this study which should be considered when interpreting our findings. We examined the effect of a previous psychiatric hospitalization on mortality following first hospitalization for NCCP over a 15-year period, in an entire country, using routinely collected morbidity and mortality data. Using a 10-year look back period, we are confident that we have identified all incident NCCP hospitalizations and excluded patients with a previous hospitalization for IHD or NCCP. Hospital morbidity data are routinely audited by ISD on a 4-yearly cycle. The accuracy of a diagnosis coded in the principal diagnostic position is high and has been consistently so throughout the study period.26 We are, however, only able to identify individuals hospitalized with NCCP. This group may not be representative of all patients with NCCP. Over time, the risk stratification of patients presenting to hospital with chest pain has been optimized which may have increased the sensitivity of a NCCP diagnosis. There have been significant changes in the structure of, and access to, health care services, in particular the growth of RACPC.27 This may have had an impact on the probability of a patient with NCCP being hospitalized. To account for this, we were able to adjust for year of hospitalization in our analyses. Despite these developments, an ever increasing number of people in Scotland are presenting, being assessed and diagnosed with NCCP outside these services. Our population-based study of patients hospitalized with NCCP therefore makes a significant contribution to the literature in this area.
In a representative sample of the Scottish population, the prevalence of possible psychiatric disorder, as measured by the General Health Questionnaire (GHQ12), was estimated in 2008 to be 17% in women and 12% in men.28 Published reports suggest that psychiatric morbidity is much higher in patients with NCCP, ranging from 36 to 61%.2,13,15,19 We examined patients who had a previous psychiatric hospitalization and are therefore, by definition, likely to have had at least one episode of severe mental illness. This may explain the low prevalence of pre-existing psychiatric disorder in our study relative to population estimates and published reports. It is unclear to what extent prevalent psychiatric conditions that do not necessitate hospitalization may influence mortality risk.
The proportion of patients with a psychiatric disorder that are hospitalized under a mental health specialty in Scotland is not known. Over time, there have been significant changes to the structure of mental health services in Scotland which may have had an impact on the threshold for psychiatric hospitalization. Indeed, the Scottish Government has made a policy commitment to transferring the balance of psychiatric care from hospitals to the community29 and since 1980 there has been a continuous reduction in the rate of first psychiatric hospitalizations in women, while rates in men have remained stable.30 We believe, however, that any misclassification of patients would bias our findings towards the null and underestimate the true association between psychiatric disorder and mortality.
These analyses were carried out on an administrative data set with limited clinical and therapeutic data. We are therefore unable to determine the influence of social, behavioural, lifestyle, or physiological parameters often associated with psychiatric disease on the elevated mortality risk we report.
Conclusions
Patients discharged from hospital with NCCP in Scotland are at measurable risk of death, all-cause and CVD-specific, within a year of initial presentation. In both men and women, independent of SED, previous psychiatric hospitalization is associated with short-term all-cause and CVD-specific mortality; the youngest patients experiencing the greatest relative risk. Improved risk assessment of patients discharged from hospital with NCCP is required. Research to understand the factors that independently mediate excess risk in patients with severe mental illness, and in turn strategies to modify risk, are urgently required.
Ethical approval
This study complies with the declaration of Helsinki. This study used fully anonymized data from a routinely linked national dataset. Ethical review was not required.
Funding
There was no specific funding for this project; however, G.D.B. is a Wellcome Trust Career Development Fellow (WBS U.1300.00.006.00012.01).
Conflict of interest: none declared.
Acknowledgements
All authors formulated the study hypothesis and developed analyses plan. M.G., K.M.T., and P.S.J. carried out statistical analyses. All authors participated in interpretation of the data. M.G. drafted the manuscript with input from other authors.


{kind=link}
{kind=link}
{kind=link}
{kind=link}